Meniscectomie
De KNGF-richtlijn Meniscectomie omvat het fysiotherapeutisch diagnostisch en therapeutisch proces bij patiënten die een primaire (artroscopische of artrotomische) meniscectomie hebben ondergaan.
Publicatiedatum: 1 maart 2006
Modulaire herziening: 1 oktober 2017 (B.3. update klinimetrie)

Algemene informatie
Inleiding
De ‘KNGF-richtlijn Meniscectomie’ omvat het fysiotherapeutisch diagnostisch en therapeutisch proces bij patiënten die een primaire (artroscopische of artrotomische) meniscectomie hebben ondergaan.
De ‘KNGF-richtlijn Meniscectomie’ is een leidraad voor het fysiotherapeutisch handelen bij patiënten na een primaire meniscectomie. In de richtlijn worden het diagnostisch en therapeutisch proces beschreven conform het methodisch fysiotherapeutisch handelen.
Definitie
Een KNGF-richtlijn is gedefinieerd als ‘een systematisch ontwikkelde, vanaf centraal niveau geformuleerde leidraad, die door deskundigen is opgesteld en die is gericht op de inhoud van het methodisch fysiotherapeutisch handelen bij bepaalde gezondheidsproblemen en op (organisatorische) aspecten die met de beroepsuitoefening te maken hebben’.1,2
A.1 Doelstelling en doelgroep
De richtlijn is bedoeld voor fysiotherapeuten in de eerste en de tweede lijn en richt zich op de postoperatieve behandeling na een primaire meniscectomie.
Van de fysiotherapeuten die werken volgens de richtlijn wordt verwacht dat zij kennis hebben van ongevalmechanismen in relatie tot de aard van de letsels, aangedane structuren, functies en vaardigheden, diagnostische tests en het beloop van het functionele (weefsel)herstel. Daarnaast is kennis vereist over ‘kwaliteit van bewegen’ (o.a. het dynamisch gangpatroon) en trainingsleer en is ervaring met het toepassen van specifieke oefenvormen van belang. Voor de sportspecifieke revalidatie van maximale sporters (topsporters) en prestatiesporters zijn in de regel competenties op het niveau van de sportfysiotherapeut vereist.
Een voorwaarde voor het kunnen toepassen van de richtlijn is een goed geoutilleerde praktijk en de aanwezigheid van een oefenzaal c.q. ruimte die groot genoeg is om een analyse van het gaan en andere loopvormen te doen en om in meer belastende oefensituaties te kunnen oefenen. Er kunnen meerdere patiënten tegelijk in een oefenzaal (volgens hun individuele doelstellingen) oefenen; zij worden hierbij echter altijd individueel begeleid.
Doelstelling
De doelstelling van de richtlijn is het beschrijven van de ‘optimale’ fysiotherapeutische zorg met betrekking tot doeltreffendheid, doelmatigheid en zorg op maat bij patiënten na een meniscectomie, gebaseerd op de huidige wetenschappelijke, beroepsinhoudelijke en maatschappelijke inzichten. Deze zorg moet leiden tot een volledig (of gewenst) niveau van activiteiten en participatie en het voorkomen van chronische klachten en recidieven. De KNGF-richtlijn is daarnaast expliciet bedoeld om:
- de zorg op basis van huidige wetenschappelijke inzichten in de gewenste richting te veranderen;
- de uniformiteit en de kwaliteit van de zorg te verhogen;
- de taken en verantwoordelijkheden van beroepsgroepen af te bakenen, inzichtelijk te maken;
- de onderlinge samenwerking te stimuleren;
- de fysiotherapeut te ondersteunen bij het nemen van beslissingen ten aanzien van wel of niet behandelen en bij het toepassen van diagnostische en therapeutische handelingen.
Doelgroep
Om de richtlijn toe te kunnen passen, worden aanbevelingen geformuleerd in termen van deskundigheidseisen die noodzakenoodzakelijk zijn om volgens de richtlijn te kunnen handelen. Globaal wordt gesteld dat recreatiesporters door de algemeen fysiotherapeut behandeld kunnen worden. Bij prestatiesporters stelt het Landelijk Platform Sportfysiotherapie (LPS) dat de competenties van de sportfysiotherapeut vooral nodig zijn bij het behandelen van langdurige blessures, terwijl de sportfysiotherapeut in de regel altijd de behandelaar is bij maximale (top)sporters. In het kader van specifieke voorlichting en vraagstellingen over preventie kunnen, afhankelijk van de situatie, competenties op het niveau van sportfysiotherapeut vereist zijn bij alle typen sporters.
De werkgroep beveelt deze indeling aan voor de onderlinge samenwerking en doorverwijzing tussen een algemeen fysiotherapeut en sportfysiotherapeut. Verantwoord omgaan met de grenzen van de eigen competenties en op tijd doorverwijzen naar een collega worden als essentiële en vanzelfsprekende attitude beschouwd.
A.2 Afbakening meniscectomie en epidemiologische gegevens
A.2.1 Meniscusletsels
De richtlijn gaat over de behandeling van patiënten die een primaire (artroscopische of artrotomische) meniscectomie hebben ondergaan. Meniscectomieën met gebruik van laser, meniscusreparaties en meniscustransplantaties vallen buiten het aandachtsgebied van de richtlijn.
Hetzelfde geldt voor operaties waarbij tegelijkertijd een kruisbandreconstructie heeft plaatsgevonden. Voor de behandeling van acute knieletsels en artrose van de knie wordt verwezen naar respectievelijk de KNGF Evidence Statement Acuut Knieletsel en de KNGF-richtlijn Artrose heup-knie. Idealiter wordt de richtlijn toegepast als de instroom plaatsvindt binnen tien dagen na de operatie.
Risicofactoren voor het krijgen van meniscuslaesies zijn sporten en pre-existente problemen met betrekking tot de knie (bijvoorbeeld degeneratieve verschijnselen).
A.2.2 Epidemiologie
Meniscuslaesies komen veelvuldig voor. In 2004 werden in Nederland 38.023 meniscectomieën uitgevoerd.
A.2.3 Operatietechnieken
Er zijn diverse operatieve technieken ontwikkeld om de problemen te verhelpen. De meest gangbare operatie is de partiële meniscectomie. In meer dan 95 procent van de gevallen gebeurt dit artroscopisch. In 72 procent van de gevallen wordt de mediale meniscus geopereerd.
De werkgroep formuleerde de volgende aanbeveling:
(1) Operatietechnieken
Het is aangetoond dat partiële meniscectomie de voorkeur heeft boven totale meniscectomie (o.a. vanwege kortere operatieduur, sneller postoperatief herstel).
A.2.1 Meniscusletsels
Een meniscusletsel kan het gevolg zijn van een trauma, maar het letsel kan (vooral bij oudere mensen) ook ontstaan bij min of meer normale bewegingen zonder (artrosegerelateerd) aanwijsbaar letsel. Het bekendste voorbeeld van een meniscusletsel is het ‘voetbalknietje’. De mediale meniscus is vaker aangedaan dan de laterale; de verhouding is ongeveer 75:25 procent.11 Dit heeft te maken met het feit dat de mediale meniscus sterk is verankerd aan de mediale collaterale band, waardoor ze in mechanische zin kwetsbaarder is.
In de literatuur worden verschillende soorten scheuren gedefinieerd, namelijk:
- de lengtescheur (voorkant of achterkant);
- de ‘bucket handle’ scheur (lengtescheur van achter naar voren);
- de dwarse scheur en
- de flapscheur.12
Combinaties van scheuren komen ook voor. Aan de bucket handle scheur liggen over het algemeen meerdere traumatische momenten ten grondslag.
Risicofactoren zijn determinanten of etiologische factoren die bijdragen aan het ontstaan van het gezondheidsprobleem (hier: de meniscusleasie). Ze kunnen een positieve of negatieve invloed hebben.13Risicofactoren voor meniscusleasies zijn: sporten en pre-existente problemen met betrekking tot de knie, zoals preoperatieve degeneratieve verschijnselen of preoperatieve artrose.14-22
A.2.2 Epidemiologie
De incidentie van meniscusscheuren is ongeveer 0,7 per 1000 personen per jaar.23 Bij mannen is de incidentie hoger (0,9 per 1000) dan bij vrouwen (0,4 per 1000).11 In 2004 werden in Nederland 38.023 meniscectomieën uitgevoerd (waarvan 23.555 bij mannen).24
A.3.3 Operatietechnieken
Geheel of gedeeltelijk verwijderen van de meniscus
Met het toenemen van de kennis over mogelijke schadelijke gevolgen van het geheel of gedeeltelijk verwijderen van de meniscus (‘Fairbank-changes’) is het beleid bij meniscusletsels conservatiever geworden.25 De meest voorkomende operatie is een artroscopische partiële meniscectomie.26,27 Het is aangetoond dat langetermijnresultaten van partiële meniscectomie beter zijn dan die van totale meniscectomie.28 Vooral patiënten met functionele degeneratieve verschijnselen en artrose van de knie zouden betere resultaten hebben na een partiële meniscectomie, hoewel de resultaten bij een degeneratief meniscusletsel in het algemeen slechter zijn dan bij een traumatisch letsel.19,29,30
Verder is de prognose beter en het herstel sneller als (alleen) een stabiele perifere meniscusrand wordt bewaard.31Dit wordt ook wel subtotale meniscectomie genoemd.32 Tevens is beschreven dat de haemarthros geringer is als de (goed gevasculariseerde) buitenrand van de meniscus gespaard blijft. De grootte van de incisies kan van invloed zijn op het al dan niet optreden van inhibitie van de musculus quadriceps femoris.33
Artroscopisch of artrotomisch opereren
De operatietechniek zelf heeft zich in de loop der tijd ontwikkeld. Vroeger werden vooral artrotomische operaties uitgevoerd, tegenwoordig vooral de artroscopische meniscectomie. In 1998 werd in Nederland de meniscus in 96 procent van de gevallen artroscopisch verwijderd en in 4 procent van de gevallen via een artrotomie.34 Uit een systematische review is gebleken dat er te weinig gerandomiseerde studies zijn over de resultaten na meniscusoperaties om wetenschappelijk verantwoorde conclusies over artroscopie versus artrotomie op lange termijn te trekken.28
De resultaten van artroscopische operaties lijken wel beter dan die van artrotomische operaties, omdat de minder invasieve aanpak het revalidatieproces op korte termijn versnelt.28,35-37
Transplantatie/hechten
Marti et al. hebben vastgesteld dat voor meniscustransplantatie nauwelijks indicaties bestaan.38 Omdat in Nederland nog relatief weinig meniscustransplantaties worden uitgevoerd, zijn deze buiten de richtlijn gehouden. Operaties met behulp van laser en meniscusreparaties zijn om dezelfde redenen eveneens niet in de richtlijn opgenomen.
Op basis van bovenstaande formuleerde de werkgroep de volgende aanbeveling:
(1) Operatietechnieken (niveau 1)
Het is aangetoond dat partiële meniscectomie de voorkeur heeft boven totale meniscectomie (o.a. vanwege kortere operatieduur, sneller postoperatief herstel). Kwaliteit van de gevonden artikelen: A1 (Howell & Handoll, 200228).
A.3 Gevolgen van een meniscectomie
A.3.1 Gezondheidsprobleem
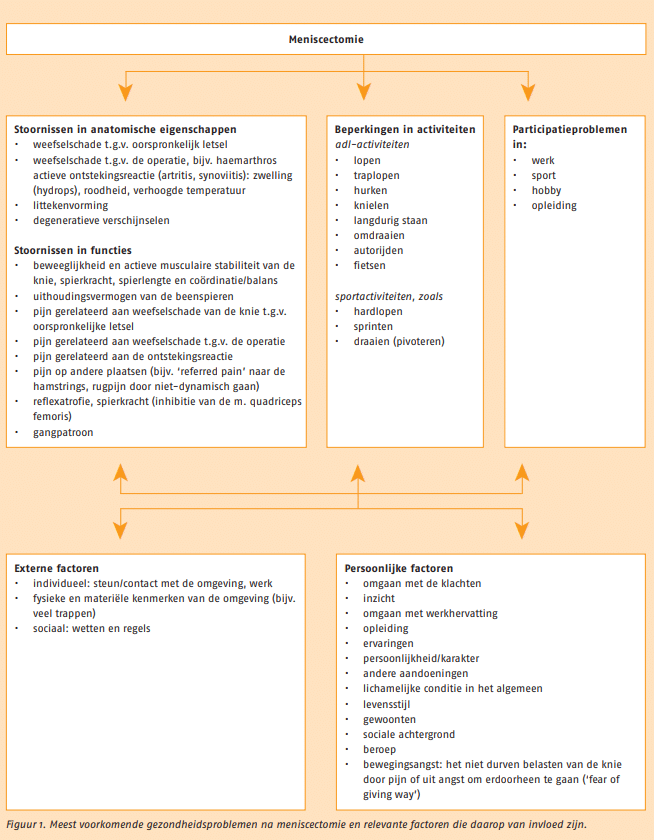
De belangrijkste gezondheidsproblemen en aandachtsgebieden na een meniscectomie staan samengevat in de volgende figuur.
A.3.2 Artrose
Na een meniscectomie is de kans op vroegtijdige ontwikkeling van artrose verhoogd. Het is aannemelijk dat totale verwijdering vaker tot vroegtijdige artrose lijdt dan partiële.
Op basis van bovenstaande formuleerde de werkgroep de volgende aanbevelingen:
(2) Artrose
Het is aangetoond dat 24 tot 42 procent van de patiënten bij een gemiddelde folluw-up van 13 jaar gonartrose ontwikkelt.
(3) Artrose
Het is aannemelijk dat op termijn artrose voorkomt, zowel bij patiënten die met de open (artrotomische) als bij patiënten die met de artroscopische techniek zijn geopereerd.
(4) Artrose
Het is aannemelijk dat totale meniscectomie vaker tot artrose leidt dan partiële meniscectomie.
A.3.1 Gezondheidsprobleem
De meniscus heeft in de knie diversie functies:39,40
- vergroting van het contactoppervlak tussen femur en tibia door vergroting van de congruentie, waarmee ook de belastingsverdelende functie samenhangt;
- stabilisatie van het gewricht;
- bewegingsbeheersing tijdens flexie en extensie;
- smering en voeding van het gewrichtskraakbeen;
- schokabsorptie.
Na een meniscectomie wordt het functioneren van een van de menisci verstoord, hetgeen kan leiden tot verschillende gezondheidsproblemen. De meest voorkomende gezondheidsproblemen na meniscectomie zijn in de volgende figuur beschreven met behulp van de ‘International Classification of Functioning, Disability and Health’ (ICF; Internationale Classificatie van het Menselijk Functioneren).41
Er is een wisselwerking tussen de stoornissen in anatomische eigenschappen en in functies, beperkingen in activiteiten, participatieproblemen en externe en persoonlijke factoren. In de paragrafen over het diagnostisch en het therapeutisch proces wordt het diagnosticeren en behandelen van deze gezondheidsproblemen uitgebreid beschreven. Behandeldoelen en verrichtingen worden opgesteld aan de hand van het gezondheidsprofiel van de patiënt.
In het algemeen zijn de doelen gelegen in het verminderen van de pijn, stoornissen in functies en anatomische structuren en het verbeteren van activiteiten en participatie.42 Verrichtingen bestaan uit informatie, voorlichting, advies, oefenen van functies, activiteiten. Zie de casussen in bijlage 2 (opent in nieuw tabblad) van de Praktijkrichtlijn.
A.3.2 Artrose
Een van de mogelijke gevolgen van meniscectomie op langere termijn is het vroegtijdig ontwikkelen van artrose. In de literatuur wordt veelvuldig melding gemaakt van het optreden van degeneratieve gewrichtsveranderingen na een meniscectomie. Gillquist en Messner toonden in een review aan dat na een meniscectomie 24 tot 42 procent van de patiënten bij een gemiddelde follow-up van 13 jaar gonartrose ontwikkelt.43 Andere auteurs vonden bij 43 procent van de patiënten artrose, 16 jaar na de meniscectomie.16 Zij concludeerden ook dat patiënten die een meniscectomie ondergaan een hoger risico hebben op artrose (Relatief Risico (RR) = 7,0; 95%-betrouwbaarheidsinterval (95%-BI) = 2,1-23,5) dan de gematchte controlegroep.
Zowel bij patiënten die een meniscectomie door middel van artrotomie als bij patiënten die een artroscopische meniscectomie hebben gehad, komt artrose voor.18,25,31,32,38,39,44-50 Een totale meniscectomie leidt op lange termijn vaker tot artrose dan een partiële.29,32,38,51 Van de door Englund en Lomander onderzochte patiënten ontwikkelde 56 respectievelijk 42 procent artrose (odds ratio = 3,6; 95%-BI = 1,4-9,4).51 Andere auteurs konden niet aantonen dat een totale meniscectomie op lange termijn vaker tot artrose leidt; zij concludeerden wel dat subjectieve en functionele uitkomsten beter zijn na een partiële meniscectomie dan na een totale verwijdering.52 Bij vergelijking van patiënten (met geopereerde knieën) met patiënten (met gezonde knieën) blijkt dat 12 tot 15 jaar na de operatie in knieën met partiële meniscectomie vier keer vaker artrose voorkomt dan in gezonde knieën en in knieën met subtotale meniscectomie zeven keer vaker.32
Jones et al. zagen bij patiënten met degeneratieve meniscuslaesies significant prominentere artrotische verschijnselen, onder meer een significante versmalling van de gewrichtsspleet, dan bij patiënten met een traumatische laesie.44 Patiënten die na een meniscectomie artrose ontwikkelen (i.e. secundaire artrose) blijken individueel sterk te verschillen wat betreft pijn, functioneren en kwaliteit van leven.53 Als risicofactoren voor het ontstaan van secundaire artrose worden genoemd: hogere leeftijd30,32,54, overgewicht, vrouwelijk geslacht51, standsafwijkingen van de knie (varus- of valgusstand)30,38,44, pre-existente kraakbeen- of gewrichtsbeschadiging30,38,51, instabiliteit38 en ook (andere) knieoperaties55. De lokalisatie en het type ruptuur en het activiteitenniveau hebben geen aantoonbare invloed op het ontstaan van secundaire artrose na een meniscectomie.29
Hoewel direct en meetbaar resultaat van de behandeling met betrekking tot artrose niet te verwachten is, kan het van belang zijn (vooral bij patiënten bij wie risicofactoren aanwezig zijn) om, naast het beoogde directe functieherstel, randvoorwaarden te scheppen ter beperking van het risico op secundaire artrose als gevolg van de operatie zo veel mogelijk te beperken. Hierbij nemen het corrigeren van standsafwijkingen, het normaliseren van het gangpatroon en actieve stabilisatie van het kniegewricht een belangrijke plaats in.
Op basis van bovenstaande formuleerde de werkgroep de volgende aanbevelingen:
(2) Artrose (niveau 1)
Het is aangetoond dat 24 tot 42 procent van de patiënten bij een gemiddelde folluw-up van 13 jaar gonartrose ontwikkelt.
Kwaliteit van de gevonden artikelen: A1 (Gillquist & Messner, 199943).
(3) Artrose (niveau 2)
Het is aannemelijk dat op termijn artrose voorkomt, zowel bij patiënten die met de open (artrotomische) als bij patiënten die met de artroscopische techniek zijn geopereerd.
Kwaliteit van de gevonden artikelen: B en C (B: Hoser et al., 200150; Maletius & Messner, 199648, Marti et al., 199338; Bolano & Grana, 199347; Hede et al., 199231; Wroble et al., 199246; Hamberg et al., 198345; Jones et al., 197844 en C: Chatain et al., 200118; Cleef, 199739,49; Rockborn & Gillquist, 199632; Fairbank, 194825).
(4) Artrose (niveau 2)
Het is aannemelijk dat totale meniscectomie vaker tot artrose leidt dan partiële meniscectomie.
Kwaliteit van de gevonden artikelen: B (Englund & Lomander, 200451; Roos et al., 199829; Rockborn & Gillquist, 199632; Marti et al., 199338).
A.4 Prognose
A.4.1 Prognostische factoren
Voor meniscectomie is uit de literatuur een aantal prognostische factoren voor herstel bekend, namelijk belemmerende en bevorderende factoren. Deze staan in de volgende tabel.
Prognostische factoren voor herstel na een meniscectomie.
Bevorderende prognostische factoren
- Participatie in sport (preoperatief)
- Goede voorbereiding op sport (postoperatief)
Belemmerende prognostische factoren
- Gecompliceerd letsel
- Plaats resectie
- Hoeveelheid verwijderd weefsel (veel)
- Financiële compensatie van werkgever
- Eerder knieoperatie(s)
- Preoperatieve pijn
De factoren zijn omkeerbaar, dat wil zeggen dat ‘gecompliceerd letsel’ een belemmerende factor is en ‘niet gecompliceerd letsel’ een bevorderende. De invloed van leeftijd en geslacht als prognostische factoren is niet duidelijk.
A.4.2 Natuurlijk beloop, normaal en vertraagd herstel
Het natuurlijk beloop na een meniscectomie is afhankelijk van de lokalisatie (mediaal of lateraal), de aard van het letsel en de preoperatieve situatie (bijv. de preoperatieve duur van de klachten). Verder is van belang of er een partiële of een totale resectie heeft plaatsgevonden en of er nevenpathologie (bijv. artrose) of andere problemen aanwezig zijn. Het natuurlijk beloop wordt gekenmerkt door een toename van functies, activiteiten en participatie in de tijd, en een afname van de pijn. Binnen twee weken moet er een verbetering te zien zijn; vanaf ongeveer zes weken na de meniscectomie moet de patiënt weer normaal adl-activiteiten kunnen uitvoeren.
Bij normaal herstel volgen patiënten het natuurlijk beloop. Bij vertraagd herstel zien we dat de functies, activiteiten en participatie niet toenemen, maar gelijk blijven of afnemen en dat de pijn en eventuele andere stoornissen toenemen of gelijk blijven (patiëntenprofiel 1).
A.4.1 Prognostische factoren
In de volgende tabel staan de prognostische factoren voor herstel na een meniscectomie vermeld, inclusief de bewijskracht. De prognostische factoren zijn ingedeeld in belemmerende en bevorderende factoren.
Indeling naar bewijskracht van prognostische factoren voor herstel na een meniscectomie.
| Prognostische factor voor herstel* | Auteurs | Niveau | Aanbeveling | |
|---|---|---|---|---|
| Bevorderend | preoperatieve participatie in sport, (fysieke, functionele status, trainingstoestand) | Chatain et al., 200118 | C | Er zijn aanwijzingen dat preoperatieve participatie in sport bijdraagt aan het herstel. |
| Katz et al., 199256 | C | |||
| Breederveld, 198857 | C | |||
| (postoperatieve) goede voorbereiding op sport | Breederveld, 198857 | C | Er zijn aanwijzingen dat patiënten die na de operatie het (weer gaan) sporten goed voorbereiden (goede kwaliteit kleding, schoeisel, ondergrond) beter herstellen. | |
| Belemmerend | plaats resectie (posterior deel of meniscusrand) | Chatain et al., 200118 | C | Er zijn aanwijzingen dat de plaats van de resectie (posterior deel of van de meniscusrand) een ongunstige factor voor herstel is. |
| Hede et al., 199231 | A2 | |||
| hoeveelheid verwijderd meniscusweefsel | Zarins et al., 199533 | B | Er zijn aanwijzingen dat patiënten waarbij veel weefsel is weggehaald een slechter herstel hebben. | |
| eerdere knieoperaties | Ferkel et al., 198522 | C | Er zijn aanwijzingen dat patiënten met eerdere knieoperaties een slechter herstel hebben. | |
| gecompliceerd letsel (meerdere scheuren) | Ferkel et al., 198522 | C | Er zijn aanwijzingen dat het hebben van een gecompliceerd letsel een belemmerende factor is voor herstel. | |
| Hulet et al., 200136 | C | |||
| financiële compensatie van de werkgever (workers compensation) | Katz et al., 199256 | C | Er zijn aanwijzingen dat financiële compensatie van de werkgever belemmerend (!) is voor herstel (begeleiden naar werk toe werkt beter). | |
| preoperatieve pijn | Moffet et al., 199458 | C | Er zijn aanwijzingen dat de hoeveelheid pijn kort voor de operatie een ongunstige factor voor herstel is. | |
| Onduidelijk: leeftijd | ouderen hebben een slechtere prognose | Menetrey et al., 200217 | C | Er is tegenstrijdig bewijs dat leeftijd een prognostische factor voor herstel is. |
| Chatain et al., 200118 | C | |||
| Crevoisier et al., 200120 | C | |||
| Rockborn & Gillquist, 199632 | C | |||
| Moffet et al., 199458 | C | |||
| Del Pizzo & Fox, 199021 | C | |||
| Paré et al., 198914 | C | |||
| Breederveld, 198857 | C | |||
| leeftijd is geen prognostische factor | Higuchi et al., 200135 | C | ||
| Hulet et al., 200136 | C | |||
| Burks et al., 199759 | B | |||
| Onduidelijk: geslacht | vrouwen hebben een slechtere prognose | Hulet et al., 200136 | C | Er is onvoldoende en tegenstrijdig bewijs dat geslacht een prognostische factor voor herstel is. |
| geslacht is geen prognostische factor | Burks et al., 199759 | C | ||
| Roos et al., 200060 | C |
A.4.2 Natuurlijk beloop, normaal en vertraagd herstel
Het natuurlijk beloop bij knieletsel is in het algemeen gunstig.9 Bij meniscectomie wordt het natuurlijk beloop gekenmerkt door een toename in functies, activiteiten en participatie in de tijd en een afname van de pijn binnen twee weken na de operatie; binnen twee weken moet er een aanzienlijke verbetering te zien zijn en vanaf ongeveer zes weken moet de patiënt weer normaal adl-activiteiten kunnen uitvoeren. Op korte termijn zijn de resultaten na een meniscectomie meestal goed: 80 tot 85 procent van de patiënten rapporteert goede tot uitstekende functionele resultaten.61-63 Op lange termijn (5-15 jaar) heeft 56 tot 83 procent van de patiënten een goed of uitstekend functioneel resultaat.36,50,64,65 Op lange termijn komen degeneratieve verschijnselen en reoperaties wel vaker voor.50
Bij normaal herstel volgen patiënten het natuurlijk beloop, wat uiteindelijk zal lijden tot volledig functioneel herstel. Vooraf is niet altijd te bepalen of een volledig functieherstel mogelijk is. Vaak zal dit pas tijdens de revalidatie blijken. Hoe dichter bij een ‘volledig herstel’, hoe kleiner de kans op recidiefletsel, chronische klachten en/of secundair letsel.
Bij vertraagd herstel nemen functies, activiteiten en participatie niet of onvoldoende toe, blijft de patiënt klachten houden en neemt de pijn niet af. Een of meerdere belemmerende factoren dragen bij aan het vertraagde herstel.
Het achterhalen van de belemmerende en bevorderende factoren is van groot belang om een goede inschatting te kunnen maken over normaal of vertraagd herstel.
A.5 Patiëntenprofielen
De mate van herstel na een meniscectomie verschilt van patiënt tot patiënt. Globaal zijn er twee uitersten. Aan de ene kant is er de patiënt die na een meniscectomie nauwelijks klachten heeft en (al dan niet begeleid) snel herstelt (bijvoorbeeld de jonge goedgetrainde sporter die bij een ongecompliceerd letsel soms al na een week weer op het sportveld te zien is (patiëntenprofiel 1); aan de andere kant de patiënt met een veel langduriger revalidatietraject met een vertraagd herstel; bijvoorbeeld iemand met een belaste voorgeschiedenis en degeneratieve verschijnselen in de knie (patiëntenprofiel 2).
Het patiëntenprofiel is van invloed op de invulling, de duur en de frequentie van de behandeling. Indien bijvoorbeeld artrosecomponenten of angst voor bewegen/ belasten op de voorgrond staan tijdens het diagnostisch proces, zal tijdens de behandeling ook de nadruk hierop komen liggen. In bijlage 2 (opent in nieuw tabblad) zijn twee casussen opgenomen waarin het verschil in benadering tussen beide profielen naar voren komt.
Op basis van bovenstaande formuleerde de werkgroep de volgende aanbeveling:
(5) Patiëntenprofielen
Mede op basis van het natuurlijk versus het vertraagd herstel is de werkgroep van mening dat er twee patiëntenprofielen (uitersten van elkaar) zijn te onderscheiden:
-
Patiënten in profiel 1 beschikken over veel bevorderende factoren voor herstel: een acuut, meestal traumatisch, enkelvoudig letsel van de meniscus, hebben niet eerder knieklachten gehad en gaan goed om met de klachten. Deze patiënten worden kortdurend of niet behandeld.
-
Patiënten in profiel 2 beschikken over veel (een of meerdere) belemmerende factoren voor herstel; er is vaak sprake van comorbiditeit: zij hebben langdurige knieklachten (bij meervoudige en degeneratieve rupturen ontwikkeld), resulterend in een meniscectomie. Zij hebben een instabiele knie en vaak degeneratieve verschijnselen en bewegingsangst. Het beloop is vertraagd en zij hebben geen goed inzicht in hun klachten. Deze patiënten worden langdurig(er) behandeld.
Patiënten die een meniscectomie ondergaan, zijn globaal onder te verdelen in twee groepen met elk een kenmerkend profiel. Deze groepen zijn uitersten van elkaar. Bij patiënten met profiel 1 verloopt het herstel in het algemeen op een natuurlijke manier en is bij hen sprake van bevorderende prognostische factoren. Bij patiënten met patiëntenprofiel 2 verloopt het herstel vertraagd en is sprake van belemmerende prognostische factoren.
In bijlage 2 (opent in nieuw tabblad) van de Praktijkrichtlijn zijn twee casussen opgenomen waarin het verschil in benadering tussen beide profielen naar voren komt.
Patiëntenprofiel 1
Bij de patiënt met patiëntenprofiel 1 is sprake van een gelokaliseerd, enkelvoudig letsel (meestal een korte flapruptuur). Het betreft hier meestal een jeugdige patiënt met acuut letsel van de meniscus. De patiënt heeft niet eerder klachten gehad en er is geen nevenpathologie (lokaal of algemeen). De passieve en actieve stabiliteit van de knie zijn goed; de patiënt heeft doorgaans een goede conditie (lokaal en algemeen). Na de operatie, meestal een partiële artroscopische meniscectomie, zijn er bij deze patiënt weinig problemen. Er zijn geen of lichte ontstekingsverschijnselen, er is nauwelijks of geen uitgesproken pijn en er is geen inhibitie (remming) van de musculus quadriceps femoris. Normaal gezien zijn er ook weinig beperkingen in activiteiten.
Deze patiënten willen meestal graag zo snel mogelijk hun activiteiten weer opnemen en zijn daarom gemotiveerd om aan het herstel te werken. Na de operatie wordt de status opgenomen door de fysiotherapeut, die de patiënt informatie geeft over het resultaat van de operatie en het te verwachten normale herstel. De patiënt krijgt van de fysiotherapeut ook instructie over leefregels en een thuisoefenschema. Bij het merendeel van de patiënten zijn 1 tot 2 zittingen om te informeren, te adviseren en terug te koppelen voldoende. Patiënten bij wie stoornissen te lang blijven bestaan en de kwaliteit van bewegen niet optimaal is of patiënten die uiteindelijk niet het activiteitenniveau van vóór de operatie bereiken, worden verwezen voor meerdere behandelingen. Dit betreft echter een beperkte groep patiënten (patiënten met comorbiditeit, ouderen zonder degeneratieve verschijnselen, ouderen die onzeker zijn of last hebben van (bewegings)angst en niet op hun knieën durven te zitten enzovoort).
Patiëntenprofiel 2
Bij de patiënt met patiëntenprofiel 2 hebben zich, na herhaalde (micro)traumata, chronische knieklachten ontwikkeld. Uiteindelijk wordt een meniscectomie uitgevoerd, waarbij meervoudige en degeneratieve rupturen worden geconstateerd. De knie is instabiel en heeft mogelijk een afwijkende as-stand. Hoewel het niet te voorspellen is, worden na de meniscectomie bij deze patiënt meer problemen gezien. Direct na de operatie is er sprake van een ontstekingsreactie en pijn; er kan inhibitie van de musculus quadriceps femoris optreden. Deze stoornissen kunnen ook langduriger blijven bestaan. Verder kan er sprake zijn van angst om het been te belasten en/of te bewegen; er kunnen degeneratieve verschijnselen bestaan (artrose), met de daarbij behorende klachten en/of andere comorbiditeit.
De patiënten hebben vaak langdurig pijn en/of kunnen niet goed met hun klachten omgaan (er is sprake van disbalans tussen belasting en belastbaarheid). Deze patiënten zijn beperkt in hun activiteiten en het duurt lang voordat zij terug zijn op het activiteitenniveau van vóór de operatie. De fysiotherapeut behandelt en begeleidt deze patiënten om de stoornissen, beperkingen en problemen met de participatie te verminderen en/of op te heffen.
Op basis van bovenstaande formuleerde de werkgroep de volgende aanbeveling:
(5) Patiëntenprofielen (niveau 4)
Mede op basis van het natuurlijk versus het vertraagd herstel is de werkgroep van mening dat er twee patiëntenprofielen (uitersten van elkaar) zijn te onderscheiden:
- Patiënten in profiel 1 beschikken over veel bevorderende factoren voor herstel: een acuut, meestal traumatisch, enkelvoudig letsel van de meniscus, hebben niet eerder knieklachten gehad en gaan goed om met de klachten. Deze patiënten worden kortdurend of niet behandeld.
- Patiënten in profiel 2 beschikken over veel (een of meerdere) belemmerende factoren voor herstel; er is vaak sprake van comorbiditeit: zij hebben langdurige knieklachten (bij meervoudige en degeneratieve rupturen ontwikkeld), resulterend in een meniscectomie. Zij hebben een instabiele knie en vaak degeneratieve verschijnselen en bewegingsangst. Het beloop is vertraagd en zij hebben geen goed inzicht in hun klachten. Deze patiënten worden langdurig(er) behandeld.
Het is van cruciaal belang een goed patiëntenprofiel van elke patiënt te maken, rekening houdend met belemmerende en bevorderende factoren voor herstel en met comorbiditeit.
A.6 Verwijzing versus Directe Toegankelijkheid Fysiotherapie (DTF)
Meniscectomieën worden uitgevoerd in dagbehandeling of tijdens een korte opname in het ziekenhuis. In de klinische fase is de fysiotherapeutische behandeling beperkt, mede door die korte opnameduur. Na de operatie wordt de patiënt gecontroleerd en geïnformeerd door de specialist over het verloop van de operatie.
Patiënten kunnen zich vervolgens met een verwijzing door een huisarts c.q. medisch specialist melden bij de fysiotherapeut (zie paragraaf A.6.1) of dit op eigen initiatief doen (Directe Toegankelijkheid Fysiotherapie (DTF)) (zie paragraaf A.6.2).
De werkgroep is van mening dat vooral patiënten met langdurige preoperatieve klachten, eventuele artrotische verschijnselen van de knie, spieratrofie (links-rechtsverschil), patiënten die slecht lopen, irrationele angst voor bewegen hebben en zij die lijden aan relevante comorbiditeit door de fysiotherapeut gezien zouden moeten worden, evenals patiënten die belang hebben bij een snelle re-integratie. De werkgroep adviseert deze groepen patiënten actief ‘in de gaten te (laten) houden’.
Meniscectomieën vinden plaats in dagbehandeling of tijdens een korte ziekenhuisopname. Na de operatie kunnen patiënten via de huisarts of specialist verwezen worden naar de fysiotherapeut of op eigen initiatief (Directe Toegankelijkheid Fysiotherapie, DTF) terechtkomen bij de fysiotherapeut. Indien de patiënt is verwezen, geldt de situatie zoals beschreven in paragraaf A.6.1.
Als de patiënt op eigen initiatief bij de fysiotherapeut komt, geldt de situatie zoals beschreven in paragraaf A.6.2 en moet screening op ‘pluis/niet-pluis’ plaatsvinden.
A.6.1 Verwijzing en aanmelding
Indien de patiënt zich met een verwijzing van een arts bij de fysiotherapeut aanmeldt, zijn, behalve de algemene verwijsgegevens, minimaal de volgende verwijsgegevens van belang:
- de operatietechniek;
- de lokalisatie en de lengte van de meniscusruptuur en de omvang van de meniscectomie;
- andere pathologie (bijv. degeneratieve verschijnselen, bandletsel, passieve stabiliteit);
- gegevens van aanvullend onderzoek;
- gebruik van medicatie;
- gebruik van loophulpmiddelen;
- percentage (partiële) belasting.
Indien noodzakelijke medische gegevens ontbreken, dient (in overleg met de patiënt) contact te worden opgenomen met de huisarts of medisch specialist. Omdat er sprake is van een verwijzing is aparte screening niet noodzakelijk en kan worden begonnen met het diagnostisch proces.
Wel moet de fysiotherapeut gedurende het diagnostisch en therapeutisch proces alert blijven op signalen en symptomen waarvoor eventueel contact met de verwijzer nodig is.
Patiënten komen op diverse momenten in het herstelproces bij de fysiotherapeut. Bij patiënten met kenmerken uit patiëntenprofiel 1 kan een eenmalig contact of enkele kortdurende contacten (informeren, adviseren, begeleiden, terugkoppelen) voldoende zijn. Bij patiënten met kenmerken uit patiëntenprofiel 2 zijn meerdere behandelingen fysiotherapie nodig. Het feit of er wel of niet wordt verwezen en het moment van verwijzen is afhankelijk van het lokale beleid. Soms vindt verwijzing plaats direct na de operatie, na het eerste controleconsult bij de medisch specialist; soms in een latere fase van herstel.
Regelmatig worden patiënten pas na zes weken door de specialist teruggezien en pas verwezen als het op dat moment niet goed gaat. Het lijkt zinvoller om bij twijfel tussentijds de fysiotherapeut al in te schakelen voor een eenmalig Consult Fysiotherapeutisch Onderzoek (CFO).66,67 De werkgroep is van mening dat vooral patiënten met langdurige preoperatieve klachten, artrotische verschijnselen, spieratrofie (links-rechtsverschil), slecht lopen, angst voor bewegen en relevante comorbiditeit moeten worden gezien door de fysiotherapeut, evenals patiënten die baat hebben bij een snelle re-integratie. Voor deze gang van zaken is een goede multidisciplinaire communicatie nodig waarin de fysiotherapeut een actieve rol heeft.
Indien de patiënt met een verwijzing van een arts bij de fysiotherapeut komt zijn, behalve de algemene verwijsgegevens, ook van belang gegevens over:
- de operatietechniek;
- de lokalisatie, het type en de omvang van de ruptuur;
- andere pathologie of comorbiditeit.
Operatietechniek
Hoewel de operatietechniek niet de belangrijkste factor voor herstel is, bepaalt de techniek artrotomisch versus artroscopisch, partieel versus totaal) mede het tempo van de genezing (en daarmee dus het tempo van de revalidatie) en het uiteindelijke resultaat. Zie voor een beschrijving van de (invloeden van de) soort operatietechniek de paragraaf A.2.
Lokalisatie, type en omvang ruptuur
De lokalisatie van de ruptuur en de omvang van de meniscectomie kunnen eveneens van invloed zijn op het tempo van de genezing. Newman et al. kwamen bijvoorbeeld tot de conclusie dat longitudinaal gelaedeerde menisci minder hun schokdempende functie verliezen dan radiair gelaedeerde menisci.68 Dit zou voor de fysiotherapeutische behandeling inhouden dat bij een longitudinale laesie sneller volledig belast kan worden. Sommige auteurs63 gaven aan dat bij meniscectomie longitudinale enkelvoudige rupturen sneller genezen dan complexe (radiaire) rupturen, terwijl andere auteurs45 geen significant verschil konden aantonen.
Hede et al. deden onderzoek naar de relatie tussen de hoeveelheid verwijderd weefsel, de lokalisatie van de ruptuur en het operatieresultaat.31 Alleen als meer dan 30 procent van het weefsel werd verwijderd, was de lokalisatie van de ruptuur van invloed op het resultaat.
Laesies aan de middenhoorn blijken beter te scoren dan laesies aan de voor- en achterhoorn. In 1998 werd in 72 procent van de gevallen de mediale meniscus geopereerd en in 28 procent van de gevallen de laterale.
Over de vraag of rupturen van de laterale meniscus beter genezen dan die van de mediale of andersom zijn de meningen verdeeld.63 Levy et al. vonden dat anteriore posteriore stabiliteit van het kniegewricht minder wordt aangetast bij een laterale meniscectomie dan bij een mediale.69 De goed gevasculariseerde buitenranden van beide menisci genezen gemakkelijker spontaan.31
Andere pathologie of comorbiditeit
Andere pathologie of comorbiditeit (bijvoorbeeld passieve instabiliteit, bandletsel, degeneratieve verschijnselen) is van invloed op het herstel na de operatie. De mate van passieve stabiliteit van de knie blijkt in sterke mate van invloed te zijn op het uiteindelijke resultaat van de operatie. Vooral met een totale meniscectomie wordt door verwijdering van de meniscus de passieve stabiliteit van de knie aangetast. Sommige studies laten zien dat het resultaat bij een meniscectomie (zowel artrotomisch als artroscopisch) slechter is en dat er meer recidieven optreden als ook de voorste kruisband insufficiënt is.21 Dit komt het sterkst tot uitdrukking bij patiënten die een hoog activiteitenniveau hebben. Als tijdens de operatie de mate van stabiliteit is beoordeeld, dient de verwijzer hiervan melding te maken op de verwijsbrief.
De klachten die het gevolg kunnen zijn van degeneratieve verschijnselen verergeren over het algemeen als gevolg van de ingreep. Verder meldt een aantal auteurs dat, als er degeneratieve verschijnselen van het gewrichtskraakbeen zijn, dit een direct verband heeft met de resultaten van de ingreep en dat dit de snelheid van het herstel nadelig kan beïnvloeden.33,54,63 Tijdens de behandeling moet de fysiotherapeut alert zijn op de aanwezigheid van degeneratieve verschijnselen. Verder is het zinvol te weten of de patiënt al dan niet volledig kan belasten en of de (oudere) patiënt voor de operatie instructie heeft gehad over het lopen met krukken.
Tot slot zijn gegevens van aanvullend onderzoek van belang voor de volledige beeldvorming, evenals informatie over het gebruik van medicatie (zowel pijnmedicatie als andere medicatie, bijvoorbeeld die voor de bloeddruk of voor comorbiditeit). Indien noodzakelijke medische gegevens ontbreken, dient contact te worden opgenomen met de huisarts of de medisch specialist. Is er tegelijkertijd met de meniscusoperatie een kruisbandconstructie uitgevoerd, dan valt de behandeling buiten de kaders van deze richtlijn.
A.6.2 Directe Toegankelijkheid Fysiotherapie
In het kader van de directe toegankelijkheid tot de fysiotherapie, die met ingang van 1 januari 2006 wettelijk mogelijk is, is het screeningsproces aan het fysiotherapeutisch methodisch handelen toegevoegd. Het screeningsproces bestaat uit vier onderdelen: aanmelding, inventarisatie van de hulpvraag, screening op pluis/niet-pluis en informeren en adviseren over de bevindingen van het screeningsproces.
Bij screenen wordt door middel van het stellen van gerichte vragen, het afnemen van tests of door het verrichten van andere diagnostische verrichtingen binnen een beperkte tijd vastgesteld of er al dan niet sprake is van een binnen het competentiegebied van de individuele fysiotherapeut vallend patroon van tekens en symptomen.
Aanmelding
Indien de patiënt op eigen initiatief komt (zonder verwijzing, directe toegankelijkheid fysiotherapie, DTF), heeft de fysiotherapeut gegevens nodig die betrekking hebben op de uitgevoerde meniscectomie, zoals (medische) gegevens over de operatietechniek, omvang van de meniscectomie (lokalisatie, lengte van de scheur), medicatiegebruik, andere pathologie, loophulpmiddelen of eerdere knieoperaties. Deze gegevens staan veelal vermeld in de ontslagbrief die de patiënt uit het ziekenhuis heeft meegekregen. De fysiotherapeut vraagt de patiënt daarom deze brief mee te nemen.
Eventueel verstrekt de patiënt aanvullende informatie. Indien de medische gegevens niet of onvoldoende duidelijk zijn, is het de verantwoordelijkheid van de individuele fysiotherapeut om (met toestemming van de patiënt) contact op te nemen met de huisarts of specialist om aanvullende informatie in te winnen.
Inventarisatie hulpvraag
Bij de inventarisatie van de hulpvraag van de patiënt is het van belang de belangrijkste klachten, het beloop van de klachten en de doelstelling voor de behandeling te achterhalen.
Screening pluis/niet-pluis
Op basis van leeftijd, geslacht, incidentie en prevalentie en de gegevens over ontstaanswijze, symptomen en verschijnselen moet de fysiotherapeut kunnen inschatten of symptomen en verschijnselen pluis of niet-pluis zijn, om te kunnen besluiten of verder fysiotherapeutisch onderzoek zonder tussenkomst van een arts geïndiceerd is.
Bij de screening is de fysiotherapeut alert op patroonherkenning en op het identificeren van eventuele aanwezige rode vlaggen (alarmsignalen). (Zie ook de differentiaaldiagnostiek in de Verantwoording).
Alarmsignalen na een meniscectomie
- persisterende onbegrepen pijn;
- (te) lage belastbaarheid van de knie (afwijkend beloop);
- ontstekingsverschijnselen als gevolg van (postoperatieve) infectie en/of
- persisterende ontstekingsverschijnselen.
Belangrijkste symptomen
- De pijn is niet provoceerbaar of reduceerbaar bij het uit oefenen van functies (bijv. aanspannen van de musculus quadriceps femoris) en het uitvoeren van activiteiten (bijv. lopen, knielen).
- De zwelling neemt niet af.
- De knie wordt niet dunner, ondanks bewegen en/of oefenen.
Informeren en adviseren
Aan het einde van het screeningsproces wordt de patiënt geïnformeerd over de bevindingen. Indien een of meerdere symptomen afwijken van een bekend patroon, het patroon onbekend is of een afwijkend beloop heeft volgens de individuele therapeut of bij aanwezigheid van rode vlaggen (conclusie: niet-pluis), wordt de patiënt geadviseerd om contact op te nemen met de huisarts. Indien de bevindingen wel pluis zijn, wordt de patiënt geïnformeerd over de mogelijkheid om door te gaan met het diagnostisch proces.
In het kader van de DTF die met ingang van 1 januari 2006 van kracht is, is het screeningsproces aan het methodisch handelen toegevoegd. Screening is een proces dat de fysiotherapeut leidt tot de beslissing of verder fysiotherapeutisch onderzoek zonder tussenkomst van een arts geïndiceerd is. Bij screenen wordt door middel van gerichte vragen, tests of andere diagnostische verrichtingen binnen een beperkte tijd (circa 10 minuten) vastgesteld of er al dan niet sprake is van een binnen het competentiegebied van de individuele fysiotherapeut vallend patroon van tekens en/of symptomen.70
Het screeningsproces bestaat uit de aanmelding, inventarisatie van de hulpvraag, screening op ‘pluis/niet-pluis’ en informeren en adviseren. Omdat patiënten na een meniscectomie veelal zullen worden verwezen, is ook screening in deze richtlijn opgenomen. Bij de andere richtlijnen die zijn gepubliceerd na 1 januari 2006, is de indeling anders (met meer nadruk op screening).
Aanmelding
Als een patiënt zich op eigen initiatief meldt na een meniscectomie, is het nodig een aantal medische gegevens te achterhalen zoals: de operatietechniek, de soort meniscectomie, medicatiegebruik, andere pathologie, loophulpmiddelen en eerdere knieoperaties. Dit kan (deels) via de patiënt (bijv. informatie over loophulpmiddelen of eerdere operaties) of via de ontslagbrief uit het ziekenhuis (niet hetzelfde als de verwijsbrief!). Vraag de patiënt deze ontslagbrief mee te nemen.
Als er naar inschatting van de individuele fysiotherapeut onvoldoende of onduidelijke medische gegevens zijn, wordt er in overleg met de patiënt contact gezocht met de huisarts of specialist. In de praktijk blijkt contact vaak noodzakelijk. Uiteraard is contact niet noodzakelijk wanneer een goede ontslagbrief voorhanden is.
Inventarisatie hulpvraag
Wat zijn de doelstellingen en verwachtingen van de patiënt?
- Wat zijn de belangrijkste klachten?
- Welke activiteiten zijn belangrijk voor de patiënt?
Inventarisatie van de hulpvraag is essentieel voor het afstemmen van het revalidatieproces. Patiënten hebben verschillende en individuele verwachtingen.71 Een atleet van 28 jaar stelt hogere eisen aan het herstel van de knie dan een man van 68 jaar. De doelstellingen van een patiënt na een meniscectomie links, met rechts pre-existent gecombineerde mediale banden kruisbandletsels zullen anders zijn dan die van een even oude patiënt met een blanco voorgeschiedenis. Verder verwachten vrouwen vaker een verbetering in het gangpatroon en mannen een verbetering tijdens sporten; jongere patiënten verwachten dat de knie weer als vanouds zal functioneren naast een verbetering tijdens sporten en oudere patiënten verwachten vaker een vermindering van pijn en een verbetering in het gangpatroon.71
Screening pluis/niet-pluis
De fysiotherapeut is bij het screenen alert op patroonherkenning en op de identificatie van eventuele alarmsignalen c.q. rode vlaggen. De patiënt wordt geadviseerd contact op te nemen met de huisarts of specialist indien: het patroon niet bekend is bij de individuele fysiotherapeut (dat zal dus op basis van scholing en ervaring per therapeut verschillen!), een of meerdere symptomen afwijken van een bekend patroon, er een afwijkend beloop is, of als er een of meerdere alarmsignalen aanwezig zijn.
Differentiaaldiagnostiek
De specifieke alarmsignalen na een meniscectomie zijn persisterende onbegrepen pijn, (te) lage belastbaarheid van de knie (afwijkend beloop), ontstekingsverschijnselen als gevolg van een infectie en/of persisterende ontstekingsverschijnselen. De belangrijkste symptomen hierbij zijn dat de pijn niet provoceerbaar of reduceerbaar is bij het uitoefenen van functies (bijv. het aanspannen van de musculus quadriceps femoris) en het uitvoeren van activiteiten (bijv. lopen, knielen), dat de zwelling niet afneemt en dat de knie niet dunner wordt, ondanks bewegen en/of oefenen. Voor een uitgebreidere beschrijving van de algemene alarmsignalen zoals koorts, (nachtelijk) transpireren, misselijkheid, (onnatuurlijke) bleekheid, duizeligheid, flauwvallen, verdenking op neurologische klachten, fracturen enzovoort wordt verwezen naar de voor DTF ontwikkelde materialen.72
Informeren en adviseren
Aan het einde van het screeningsproces wordt de patiënt geïnformeerd over de bevindingen (patroon en eventuele alarmsignalen) en geadviseerd contact op te nemen met de huisarts indien de conclusie ‘niet-pluis’ is, dat wil zeggen dat het patroon onbekend is voor de individuele fysiotherapeut, een of meerdere symptomen afwijken van een bekend patroon, er een bekend patroon is met een afwijkend beloop of er een of meerdere alarmsignalen aanwezig zijn.
De arts kan alsnog aanvullende diagnostiek verrichten c.q. aanvragen om vervolgens het te voeren beleid te bepalen. Wanneer met aanvullende informatie van de arts een voor de fysiotherapeut voldoende verklaard patroon van symptomen is ontstaan, behoort fysiotherapeutische advisering en/of behandeling tot de mogelijkheden. Indien de bevindingen wel ‘pluis’ zijn (conclusie: bekend patroon), wordt de patiënt hierover geïnformeerd en kan zonder tussenkomst van een arts worden vervolgd met het fysiotherapeutisch diagnostisch proces; de aanvullende anamnese en aanvullend onderzoek.