Enkelletsel [richtlijn]
B.2 (Aanvullend) onderzoek
Inspectie
- Waar is de pijn gelokaliseerd?
- Is er sprake van zwelling? Waar, in welke mate en wat is de kleur ervan?
- Hoe is de statiek? Zijn er standsafwijkingen?
Differentiaaldiagnostiek
Aangezien bij acuut enkelletsel een fractuur kan optreden, adviseert de werkgroep om ten behoeve van de fractuurdiagnostiek in de acute fase (tot 7 dagen na het trauma) de ‘Ottawa ankle rules’ te hanteren. Volgens deze regels is er een indicatie voor röntgendiagnostiek van de enkel of de middenvoet indien de patiënt pijn aangeeft in het malleolaire gebied en er sprake is van:
- onvermogen de enkel te belasten (vier stappen 2×2-lopen zonder hulp); of
- pijn bij palpatie van dorsale of caudale zijde van de laterale malleolus (onderste 6 cm); of
- pijn bij palpatie van dorsale of caudale zijde van de mediale malleolus (onderste 6 cm); of
- pijn bij palpatie van de basis van het os metatarsale V; of
- pijn bij palpatie van het os naviculare.
Overige onderzoeksbevindingen die verdenking op een fractuur in de middenvoet geven, zijn:
- asdrukpijn in de voorvoet of de hiel;
- drukpijn op het verloop van de fibula (de zogeheten maison neuf-fractuur).
Kleine avulsiefracturen hebben in het merendeel van de gevallen geen consequenties voor het te voeren beleid. Als de patiënt de voet binnen 48 uur na het trauma kan belasten, is de kans gering dat er sprake is van een fractuur. Het is een gunstig teken voor de ernst van het letsel en het beloop van het herstel. In de volgende figuur zijn de Ottawa ankle rules weergegeven.
De Ottawa ankle rules.
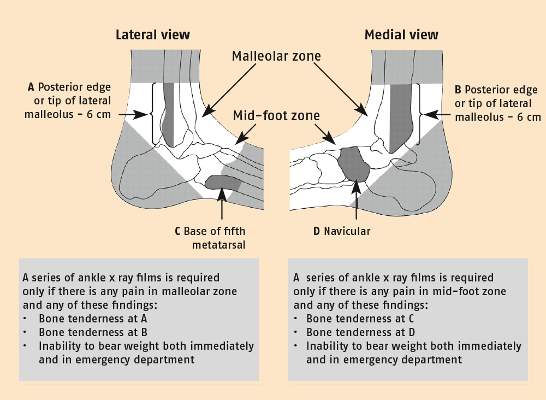
Met toestemming overgenomen uit: Bachmann LM, Kolb E, Koller MT, Steurer J, Ter Riet G. Accuracy of Ottawa ankle rules to exlude fractures of the ankle and mid-foot: systematic review. BMJ 2003;326:417-23.
Een onderzoeksbevinding die spieren/of peesletsels doet vermoeden is het onvermogen van de patiënt om de spieren van het onderbeen aan te spannen vanwege de pijn en/of vanwege onderbreking van de continuïteit van de spier en/of pees. Andere onderzoeksbevindingen die een uitgebreider letsel doen vermoeden zijn:
- hyper- of hypomobiliteit van de enkel;
- pijn aan de mediale zijde (‘kissing pain’/osteochondraal letsel).
Bij verdenking op een fractuur, spieren/of peesletsel of uitgebreidere pathologie wordt, in overleg met de patiënt, terugverwezen of overleg gepleegd met de huisarts of de specialist, die alsnog aanvullende diagnostiek kan verrichten c.q. aanvragen om vervolgens het te voeren beleid te bepalen.
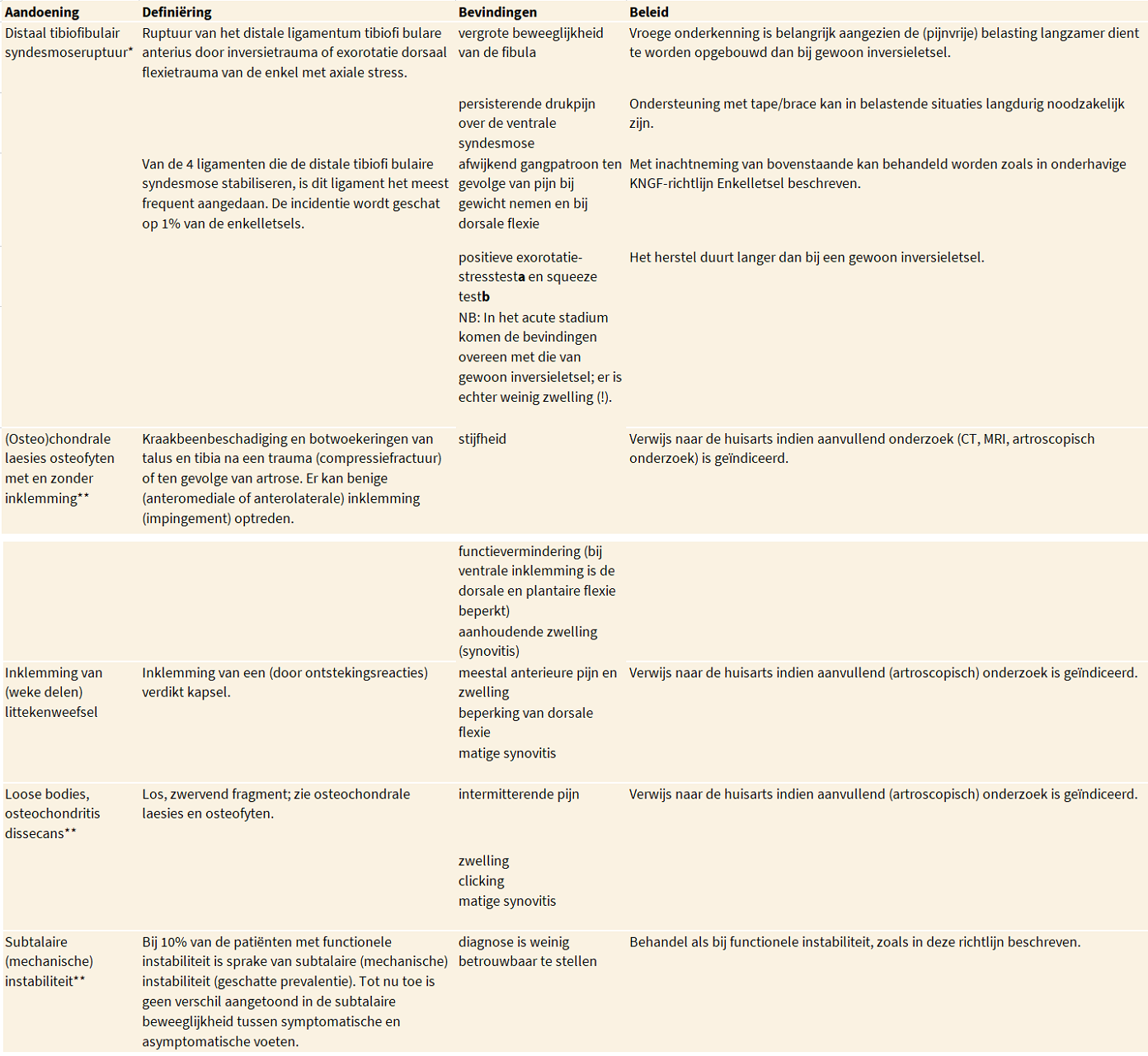
Ten behoeve van de differentiaaldiagnostiek staan in de volgende tabel de belangrijkste symptomen en het gebruikelijke beleid bij genoemde aandoeningen beschreven. Zie ook de Verantwoording van paragraaf A7.1.
Differentiaaldiagnostiek bij chronische enkelklachten.
Functieonderzoek
- Actief bewegingsonderzoek: Is actieve plantaire en dorsale flexie van de voet mogelijk?
- Passief bewegingsonderzoek: Is eventueel (belast en onbelast) passieve dorsale flexie mogelijk?
- In welke mate kan de voet worden belast?
- Is er daarbij sprake van pijn, giving way, bewegingsangst of anderszins?
- Is de patiënt in staat om op één been te staan met open c.q. gesloten ogen?
- Hoe verhouden zich de evenwichtsreacties van de aangedane tot die van de niet-aangedane zijde in stand en tijdens lopen?
Acuut enkelletsel
In verband met (sportspecifieke) revalidatie: Is er sprake van een ruptuur van het ligamentum talofibulare anterius? Het onderscheid tussen een distorsie of ruptuur kan worden gemaakt met uitgesteld fysisch diagnostisch onderzoek (4-5 dagen na trauma), namelijk: het uitvoeren van een voorste schuifladetest , het vaststellen van hematoomverkleuring en palpatiepijn van het ligamentum.
Functionele instabiliteit
- Hoe is het gangpatroon?
- Is de patiënt in staat om, na een sprong op het aangedane been, weer stil te staan op één been?
- Is de patiënt in staat om op de tenen/hakken te gaan?
- Is de patiënt in staat om hogere belastingsvormen met dubbeltaken uit te voeren?
De werkgroep formuleerde de volgende aanbevelingen:
(2 t/m 4) Passieve tests
De werkgroep is van mening dat passieve (stress)tests over het algemeen geen toegevoegde waarde hebben voor het bepalen van de fysiotherapeutische diagnose bij enkelletsel.
Er zijn aanwijzingen dat de (uitgestelde) voorste schuifladetest aanvullende informatie kan geven over de mechanische instabiliteit van de enkel.
De werkgroep is van mening dat de (uitgestelde) voorste schuifladetest alleen geïndiceerd is bij prestatiegerichte sporters en maximale sporters, ter ondersteuning van de revalidatie en verwachte terugkeer op (top)sportniveau.
(5) Gebruik van de Functiescore
Er zijn aanwijzingen dat de Functiescore een adequaat instrument is om lichte enkelletsels te onderscheiden van zware enkelletsels.
Passieve tests
De test die onderscheid kan aangeven tussen een distorsie en een ruptuur is mogelijk de voorste schuifladetest. In de acute fase na het trauma is de betrouwbaarheid en de validiteit van de test laag.20,87,88 Wanneer uitvoering ervan niet onder (lokale) verdoving plaatsvindt, zijn betrouwbaarheid en validiteit nog lager.20,87 De betrouwbaarheid is echter hoger als de schuifladetest 4 tot 7 dagen na het trauma wordt uitgevoerd, in combinatie met andere tests.20,89 Resultaten zijn dan vergelijkbaar met de resultaten van artrografie.
Uitvoering van de test zonder verdoving is waarschijnlijk in het subacute of chronische stadium beter te tolereren dan in de acute fase, omdat er in de eerstgenoemde stadia sprake is van minder pijn, zwelling en reactieve spierspanning, waardoor de betrouwbaarheid van de schuifladetest naar verwachting stijgt.20
De fysiotherapeutische relevantie van passieve tests voor het onderscheid tussen een distorsie en een ruptuur is niet duidelijk. Hubbard et al. hebben aangetoond dat bij patiënten met functionele instabiliteit een toegenomen anterior-posterior verplaatsing is waar te nemen.90 Zij hebben echter klinisch geen verschillen gevonden tussen patiënten met en zonder toegenomen anterior-posteriorverplaatsing.
Bij prestatiegerichte sporters en maximale sporters kan, indien de behoefte bestaat, de schuifladetest eventueel worden uitgevoerd ter bepaling van de mate van mechanische instabiliteit. Bij deze groep patiënten kan aanvullende informatie van belang zijn in verband met de hoge belasting van de enkel in hun sportactiviteiten.
Schuifladetest
Uitgangshouding van de patiënt:
- ruglig, het bovenbeen rust op de bank, de knie is gebogen en het onderbeen hangt af;
- in zit met afhangend been;
Omvat de hiel, ondersteun de voetzool van de patiënt met de onderarm en houd de voet in 10 tot 15 graden plantaire flexie. Omvat vervolgens met de andere hand de voorzijde van het onderbeen ongeveer 10 cm boven de enkel. Beweeg de ontspannen voet naar ventraal bij gefixeerd onderbeen.
Interpretatie: De test is positief als de voet ten opzichte van het onderbeen minstens 1 cm meer naar ventraal glijdt dan de voet aan de gezonde zijde bij het uitvoeren van dezelfde test. De patiënt moet kunnen ontspannen: de test is niet pijnlijk en de onderzoeker vertelt aan de patiënt wat er gaat gebeuren, zowel van tevoren als op het moment zelf.
Er is geen consensus in de literatuur aangaande het nut van uitvoering van talar tilt-tests. De prognostische waarde van deze tests wat betreft herstel van het letsel is gering en het te voeren beleid wordt niet beïnvloed door de resultaten van de tests. De correlatie tussen een positieve talar tilt en functionele instabiliteit is matig.90-93 Derhalve zijn deze tests niet in de richtlijn opgenomen.
Passieve tests ter lokalisatie van de pijn worden niet uitgevoerd, omdat lokale behandeling (op pijnpunten) in deze richtlijn niet wordt toegepast; in de literatuur zijn voor deze behandeling geen argumenten te vinden.
| Op basis van bovenstaande formuleerde de werkgroep de volgende aanbevelingen: (2) Passieve tests (niveau 4) (3) Passieve tests (niveau 3) (4) Passieve tests (niveau 4) |
Functiescore
De werkgroep stelt voor om bij acuut letsel het onderscheid tussen lichte en ernstiger letsels te maken aan de hand van de functiescore van De Bie et al.27 Onderscheid maken aan de hand van deze score maakt uitvoering van de schuifladetest ter bepaling van de ernst van het letsel overbodig.
Indien een patiënt binnen vijf dagen na het trauma bij de fysiotherapeut komt, kan gebruik worden gemaakt van de Functiescore.
Met behulp van deze score is de therapeut in staat om ‘lichte’ letsels te onderscheiden van ernstigere letsels. Aan de hand van bepaling van de functiescore (door de fysiotherapeut) kan bij acuut enkelletsel een prognose worden gegeven omtrent de hersteltijd. Bij patiënten met een score van meer dan 40 punten op dag 0 tot 5 na ontstaan van het letsel is sprake van een licht letsel. Zij ontwikkelen zeer snel een redelijk looppatroon, met in de meeste gevallen geringe zwelling en geringe pijn tijdens het lopen en kunnen naar verwachting binnen 14 dagen weer hun normale dagelijkse activiteiten uitvoeren.27 In het algemeen is geen specifieke fysiotherapeutische behandeling nodig, uitgaande van een normaal beloop van het herstel.
Hiervan kan worden afgeweken als er sprake is van een pre-existente instabiele enkel (recidiefletsels). Bij lichte letsels kan in het kader van sportspecifieke revalidatie van prestatiegerichte sporters en maximale sporters worden behandeld tot volledig herstel.
Patiënten met ernstige(r) letsels (≤ 40 punten) dienen wel specifiek behandeld/begeleid te worden.
| Op basis van bovenstaande formuleerde de werkgroep de volgende aanbeveling: (5) Gebruik van de Functiescore (niveau 3) |
Onderzoek van de mobiliteit van de enkel
De bewegingsuitslag die het eerst tot pijn en functionele problemen leidt bij verminderde mobiliteit is de dorsale flexie.66 Er is 20 tot 30 graden dorsale flexie nodig om te kunnen rennen.94,95 Met betrekking tot het gangpatroon is een pijnvrije bewegingsuitslag van de dorsale flexie bepalend voor de snelheid van gaan en voor de staplengte contralateraal.
Indien, naar aanleiding van de anamnese, het actief bewegingsonderzoek of de observatie van het gangpatroon, de indruk bestaat dat de dorsale flexie beperkt en/of pijnlijk is, wordt passief onderzoek van de mate van dorsale flexie aangeraden.
Beoordelen van het lopen
Uitgangspunt van de werkgroep is dat een normaal looppatroon voorwaarde is voor herstel van de enkel op stoornisniveau. Anders gezegd: een afwijkend looppatroon kan klachten van de enkel onderhouden. Herstel van het normale dynamische gaan vormt een van de subdoelstellingen van de behandeling.
Dynamisch gaan onderscheidt zich van het statisch lopen, waarbij de gewrichten meer gefixeerd zijn, en van passief lopen, waarbij de stabiliteit voornamelijk wordt verzorgd door het kapsel-bandapparaat. De specifieke kenmerken van het dynamisch lopen, afgeleid van de Ganganalyselijst Nijmegen(GALN)96 zijn:
- de stapfrequentie is 100 tot 120 stappen per minuut;
- er vindt een flexiebeweging plaats in de knie aan het begin van de standfase;
- de hak maakt als eerste contact met de vloer;
- er vindt hielheffing van het standbeen plaats voordat het contralaterale been hielcontact heeft (actieve afwikkeling);
- de romp bevindt zich boven of voor de heupen/ voeten;
- de armen zwaaien alternerend, ontspannen mee; de bewegingsuitslagen zijn gelijk;
- de bewegingsuitslagen van alle gewrichten zijn binnen de norm van het normale gaan.
Onderzoek van de proprioceptie en lokale spierkracht
Om de proprioceptie te testen, is gekozen voor het staan op één been met open en met gesloten ogen. Er dient te worden gelet op links-rechtsverschillen in houdingsreacties, met name in het frontale vlak, en op pijn.44 De fysiotherapeut dient vooraf in te schatten of deze test geschikt is voor de patiënt. Met deze test is het mogelijk zowel houdingsreacties (‘postural sway’) als de controle over het statisch evenwicht te evalueren om de afferente combinatie van perifere, vestibulaire en visuele bijdragen aan de neuromusculaire controle vast te stellen.39,42,44 Tevens maakt de neuromusculaire controle zelf onderdeel uit van de test. Deze zorgt, naast voor de verwerking van de afferente stimuli, voor de productie van een toereikende reactie.59 Door het sluiten van de ogen vervalt de visuele bijdrage en wordt er meer gevraagd van de sensorische feedback.
De volgende test bestaat uit het maken van een sprong vanuit stand op één been, waarbij de patiënt moet landen op het aangedane been. De fysiotherapeut beoordeelt de controle op het evenwicht op één been na de landing.
Om een indruk te krijgen van de kracht van plantaire en dorsale flectoren kan worden gekeken naar het komen tot stand op de hiel of tenenstand op één been waarbij links-rechtsverschillen met betrekking tot het aantal keer per minuut kunnen worden geteld.97 Deze tests kunnen eventueel na een aantal zittingen worden herhaald als instrument voor evaluatie van de therapie. Indien de patiënt wordt getraind op kracht, dient evaluatie op kracht plaats te vinden; wordt de proprioceptie getraind, dan dient evaluatie daarop te geschieden.
Bepalen van de kwaliteit van bewegen
Als voornoemde tests goed worden volbracht, kan worden gekeken naar de ‘kwaliteit van bewegen’ tijdens opdrachten met een zwaardere belasting en met dubbeltaken. Te denken valt hierbij bijvoorbeeld aan activiteiten die door de patiënt als belangrijk en problematisch worden ervaren of aan het testen van de balans op een beweeglijke ondergrond, zoals het staan op de oefenmat, oefentol of trampoline (met eventueel nog verzwarende neventaken als het gooien van een bal).
1 van Dijk CN, de Bie RA, Benink RJ, Bots RAA, Bossuyt PMM, Goudswaard AN, et al. Consensus diagnostiek en behandeling van het acute enkelletsel. Utrecht: CBO; 1999.
2 Goudswaard AN, Thomas S, Van den Bosch WJHM, van Weert HCPM, Geijer RMM. NHG-Standaard Enkeldistorsie. Huisarts Wet 2000;43:32-7.
3 Chan KM, Karlsson J. World Consensus Conference on Ankle Instability. Stockholm: isakos-FIMS; 2005.
4 Hendriks HJM, van Ettekoven H, Reitsma ER, Verhoeven ALJ, van der Wees PhJ. Methode voor centrale richtlijnontwikkeling en implementatie in de fysiotherapie. Amersfoort: Koninklijk Nederlands Genootschap voor Fysiotherapie KNGF; 1998.
5 Hendriks HJM, Bekkering GE, van Ettekoven H, Brandsma JW, van der Wees PhJ, de Bie RA. Development and implementation of national practice guidelines: a prospect for continuous quality improvement in physiotherapy. Physiotherapy 2000;86(10):535-47.
6 Roebroeck ME, Dekker J, Oostendorp RAB, Bosveld W. Physiotherapy for patients with lateral ankle sprains. A prospective survey of practice patterns in Dutch primary health care. Physiotherapy 1998;84(9):421-31.
7 Werkdocument ten behoeve van de werkconferentie LPS. Utrecht: Landelijk Platform Sportgezondheidszorg; 2006.
8 van der Wees PhJ, Hendriks HJM, Jansen MJ, Laurant MGH, Dekker J, de Bie R. Het gebruik van de richtlijn acuut enkelletsel in de praktijk. Ned Tijdschr Fysiother 2005;115(3):74-9.
9 van Aarschot L, Eechaute C, Asman S, Vaes P. Systematisch en kritisch gewogen literatuuronderzoek van de klinimetrische eigenschappen van meerdimensionale meetinstrumenten bij patiënten met chronische enkelinstabiliteit. Brussel: Vrije Universiteit Brussel; 2005.
10 Asman S, Eechaute C, van Aarschot L, Vaes P. Systematisch en kritisch gewogen literatuuronderzoek van de effectiviteit van oefentherapie bij patiënten met chronische enkelinstabiliteit. Brussel: Vrije Universiteit Brussel; 2005.
11 Tol JL. Het acute enkelletsel. Bilthoven: Vereniging Sport Geneeskunde; 2001.
12 CBO. Evidence-based richtlijnontwikkeling. Handleiding voor werkgroepleden. Utrecht: Kwaliteitsinstituut voor de gezondheidszorg CBO; 2005.
13 Mulder S, Bloemhoff A, Harris S. Ongevallen in Nederland, opnieuw gemeten. Amsterdam: Stichting Consument en Veiligheid; 1995.
14 Schmikli S, Wit MJP, Backx FJG. Sportblessures driemaal geteld: kerncijfers en trends uit landelijk onderzoek naar sportblessures in Nederland. Arnhem: NOC*NSF Breedtesport; 2001.
15 Verhagen EALM. Ankle sprains in Volleybal: players off balance? Vrije Universiteit Amsterdam; 2004.
16 Vriend I, van Kampen B, Schmikli S, Eckhardt J, Schoots W, den Hertog P. Ongevallen en bewegen in Nederland 2000-2003. Ongevalsletsels en sportblessures in kaart gebracht. Amsterdam: Stichting Consument en Veiligheid; 2005.
17 Vriend I, Schoots W, Toet H, Mulder S. Kosten en baten van enkelbraces bij voetbal. Amsterdam: Stichting Consument en Veiligheid; 2005.
18 van der Linden MW, Westert GP, de Bakker DH, Schellevis FG. Tweede nationale studie naar ziekten en verrichtingen in de huisartspraktijk. Klachten en aandoeningen in de bevolking en in de huisartspraktijk. Utrecht/Bilthoven: NIVEL/RVM; 2004.
19 van der Zee J. Continue Morbiditeits Registratie. Utrecht: NIVEL; 1993.
20 van Dijk CN. On diagnostic strategies in patients with severe ankle sprain thesis. Amsterdam: University of Amsterdam; 1994.
21 Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. J BoneJoint Surg 1991;73-A:305-12.
22 van Moppes FI, van den Hoogenband CR. Diagnostic and therapeutic aspects of inversion trauma of the ankle joint. Maastricht: Maastricht University; 1982.
23 Zeegers AVCM. Het supinatieletsel van de enkel. Resultaten (proefschrift). Utrecht: Universiteit van Utrecht; 1995.
24 Moller-Larsen F, Wethelund JO, Jurik AG, De Carvalho A, Lucht U. Comparison of three different treatments for ruptured lateral ankle ligaments. Acta Orthop Scand 1988;59:564-6.
25 Povacz P, Unger F, Miller K, Tockner R, Resch H. A randomized, prospective study of operative and non-operative treatment of injuries of the fibular collateral ligaments of the ankle. J Bone Joint Surg 1998;80-A:345-51.
26 Freeman MA, Dean MRE, Hanham IWF. The etiology and prevention of functional instability of the foot. J Bone Joint Surg 1965;47B:678-84.
27 de Bie RA, de Vet HC, van den Wildenberg FA, Lenssen T, Knipschild PG. The prognosis of ankle sprains. Int J Sports Med 1997 May;18(4):285-9.
28 Konradsen L, Olesen S, Hansen HM. Ankle sensorimotor control and eversion strength after acute ankle inversion injuries. Am J Sports Med 1998 Jan;26(1):72-7.
29 Lentell GL, Katzmann Li, Walters MR. The relationship between muscle function and ankle instability. JOSPT 1990;11:605-11.
30 Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med 1997 Jan;25(1):130-7.
31 DeMaio M, Paine R, Drez D, Jr. Chronic lateral ankle instability-inversion sprains: Part I. Orthopedics 1992 Jan;15(1):87-96.
32 DeMaio M, Paine R, Drez D, Jr. Chronic lateral ankle instability-inversion sprains: Part II. Orthopedics 1992 Feb;15(2):241-8.
33 Staples OS. Result study of ruptures of lateral ligament of the ankle. Clin Orthop 1972;85:50-8.
34 Karlsson J, Andreasson GO. The effect of external ankle support in chronic lateral ankle joint instability. An electromyographic study. Am J Sports Med 1992 May;20(3):257-61.
35 Renstrom PA, Konradsen L. Ankle ligament injuries. Br J Sports Med 1997 Mar;31(1):11-20.
36 Birmingham TB, Chesworth BM, Hartsell HD, Stevenson AL, Lapenskie GL, Vandervoort AA. Peak passive resistive torque at maximum inversion range of motion in subjects with recurrent ankle inversion sprains. JOSPT 1997;25:342-8.
37 Lentell G, Baas B, Lopez D, McGuire L, Sarrels M, Snyder P. The contributions of proprioceptive deficits, muscle function, and anatomic laxity to functional instability of the ankle. JOSPT 1995;21:206-15.
38 Louwerens JWK. The position of the rearfoot at the moment of heel contact and chronic lateral instability: a video analysis thesis. Rotterdam: Erasmus Universiteit Rotterdam; 1996.
39 Ryan L. Mechanical instability, muscle strength and proprioception in the functionally unstable ankle. Aust J Physiotherapy 1994;40:41-7.
40 Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med 1985;13:259-62.
41 Vaes PH, Duquet W, van den Broeck R. Enkeldistorsietrauma en enkelinstabiliteit. Jaarboek Fysiotherapie 1997;1-45.
42 Lephart SM, Pincivero DM, Rozzi SL. Proprioception of the ankle and knee. Sports Med 1998 Mar;25(3):149-55.
43 Forkin DM, Koczur C, Battle R, Newton RA. Evaluation of kinesthetic deficits indicative of balance control in gymnasts with unilateral chronic ankle sprains. J Orthop Sports Phys Ther 1996 Apr;23(4):245- 50.
44 Friden T, Zatterstrom R, Lindstrand A, Moritz U. A stabilometric technique for evaluation of lower limb instabilities. Am J Sports Med 1989 Jan;17(1):118-22.
45 Konradsen L, Ravn JB. Prolonged peroneal reaction time in ankle instability. Int J Sports Med 1991 Jun;12(3):290-2.
46 Leanderson J, Eriksson E, Nilsson C, Wykman A. Proprioception in classical ballet dancers. A prospective study of the influence of an ankle sprain on proprioception in the ankle joint. Am J Sports Med 1996 May;24(3):370-4.
47 Rozzi SL, Lephart SM, Sterner R, Kuligowski L. Balance training for persons with functionally unstable ankles. J Orthop Sports Phys Ther 1999 Aug;29(8):478-86.
48 Boyle J, Negus V. Joint position sense in the recurrently sprained ankle. Aust J Physiother 1998;44:159-63.
49 Garn SN, Newton A. Kinesthetic awareness in subjects with multiple ankle sprains. Phys Ther 1988;68:1667-771.
50 Glencross D, Thornton E. Position sense following injury. Sports Med Phys Fitness 1981;21:23-7.
51 Hartsell HD. The effects of external bracing on joint position sense awareness for the chronically unstable ankle. J Sport Rehab 2000;9:279-89.
52 Konradsen L, Ravn JB, Sorenson AI. Proprioception at the ankle: the effect of anaesthetic blockade of ligament receptors. J Bone Joint Surg Br 1993;75:433-66.
53 Karlsson J, Faxen E, Eriksson BI. Ankle joint ligament injuries: prevention, evaluation and treatment. Phys Rehab Med 1996;8:183-200.
54 Oostendorp RAB. Functionele instabiliteit na het inversietrauma van de enkel en voet: een effectonderzoek van pleisterbandage versus pleisterbandage gecombineerd met fysiotherapie (Functional instability after ankle sprains; a trial of taping versus taping and exercise). Geneeskunde en Sport 1987;20(2):45-55.
55 Burke D, Gandevia SC, Macefield G. Responses to passive movement of receptors in joint, skin and muscle of the human hand. J Physiol 1988 Aug;402:347-61.
56 Clarke FJ, Grigg P, Chapin JW. The contribution of articular receptors to proprioception with the fingers in humans. J Neurophysiol 1989;61:186-93.
57 Kleinrensink GJ, Stoeckart R, Meulstee J, Kaulesar Sukul DM, Vleeming A, Snijders CJ, et al. Lowered motor conduction velocity of the peroneal nerve after inversion trauma. Med Sci Sports Exerc 1994 Jul;26(7):877-83.
58 Kannus P, Alosa D, Cook L, Johnson RJ, Renstrom P, Pope M, et al. Effect of one-legged exercise on the strength, power and endurance of the contralateral leg. A randomized, controlled study using isometric and concentric isokinetic training. Eur J Appl Physiol Occup Physiol 1992;64(2):117-26.
59 Laskowski ER, Newcomer-Aney K, Smith J, Van Deursen RW. Proprioception. Sci Principals Sports Rehab 2000;11:323-40.
60 Vaes P, Van GB, Duquet W. Control of acceleration during sudden ankle supination in people with unstable ankles. J Orthop Sports Phys Ther 2001 Dec;31(12):741-52.
61 Konradsen L, Ravn JB. Ankle instability caused by prolonged peroneal reaction time. Acta Orthop Scand 1990 Oct;61(5):388-90.
62 Lofvenberg R, Karrholm J, Sundelin G, Ahlgren O. Prolonged reaction time in patients with chronic lateral instability of the ankle. Am J Sports Med 1995 Jul;23(4):414-7.
63 Brunt D, Andersen JC, Huntsman B, Reinhert LB, Thorell AC, Sterling JC. Postural responses to lateral perturbation in healthy subjects and ankle sprain patients. Med Sci Sports Exerc 1992 Feb;24(2):171-6.
64 Beynnon BD, Renstrom PA, Alosa DM, Baumhauer JF, Vacek PM. Ankle ligament injury risk factors: a prospective study of college athletes. J Orthop Res 2001 Mar;19(2):213-20.
65 Fernandes N, Allison GT, Hopper D. Peroneal latency in normal and injured ankles at varying angles of perturbation. Clin Orthop Relat Res 2000 Jun;(375):193-201.
66 Balduini FC, Vegso JJ, Torg JS, Torg E. Management and rehabilitation of ligamentous injuries to the ankle. J Sports Med 1987;4:364-80.
67 Louwerens JWK, van Linge B, de Klerk LWL, Mulder PGH, Snijders CJ. Peroneus longus and tibialis anterior muscle activity in the stance phase. Acta Orthop Scand 1995;66:517-23.
68 Bosien WR, Staples OS, Russell SW. Residual disability following acute ankle sprains. J Bone Joint Surg Am 1955 Dec;37-A(6):1237-43.
69 Tropp H. Pronator muscle weakness in functional instability of the ankle joint. Int J Sports Med 1986 Oct;7(5):291-4.
70 Wilkerson GB, Pinerola JJ, Caturano RW. Invertor vs. evertor peak torque and power deficiencies associated with lateral ankle ligament injury. J Orthop Sports Phys Ther 1997 Aug;26(2):78-86.
71 McKnight CM, Armstrong CW. The role of ankle strength in functional ankle instability. J Sport Rehab 1997;6:21-9.
72 Pope R, Herbert R, Kirwan J. Effects of ankle dorsiflexion range and pre-exercise calf muscle stretching on injury risk in Army recruits. Aust J Physiother 1998;44(3):165-72.
73 Hintermann B. Biomechanics of the unstable ankle joint and clinical implications. Med Sci Sports Exerc 1999 Jul;31(7 Suppl):S459-69.
74 Bahr R. Recent advances: Sports medicine. BMJ 2001 Aug 11;323(7308):328-31.
75 Wester JU, Jespersen SM, Nielsen KD, Neumann L. Wobble board training after partial sprains of the lateral ligaments of the ankle: a prospective randomized study. J Orthop Sports Phys Ther 1996 May;23(5):332-6.
76 Bachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G. Accuracy of Ottawa ankle rules to exlude fractures of the ankle and mid-foot: systematic review. BMJ 2003;326:417-23.
77 Leddy JJ, Smolinski RJ, Lawrence J, Snyder JL, Priore RL. Prospective evaluation of the Ottawa Ankle Rules in a university sports medicine center. With a modification to increase specificity for identifying malleolar fractures. Am J Sports Med 1998 Mar;26(2):158-65.
78 Leddy JJ, Kesari A, Smolinski RJ. Implementation of the Ottawa ankle rule in a university sports medicine center. Med Sci Sports Exerc 2002 Jan;34(1):57-62.
79 Papacostas E, Malliaropoulos N, Papadopoulos A, Liouliakis C. Validation of Ottawa ankle rules protocol in Greek athletes: study in the emergency departments of a district general hospital and a sports injuries clinic. Br J Sports Med 2001 Dec;35(6):445-7.
80 Brosky T, Nyland J, Nitz A, Caborn DN. The ankle ligaments: consideration of syndesmotic injury and implications for rehabilitation. J Orthop Sports Phys Ther 1995 Apr;21(4):197-205.
81 Hopkinson WJ, St PP, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle 1990 Jun;10(6):325-30.
82 van Dijk CN, Tol JL, Verheyen CC. A prospective study of prognostic factors concerning the outcome of arthroscopic surgery for anterior ankle impingement. Am J Sports Med 1997 Nov;25(6):737-45.
83 Shea MP, Manoli A. Osteochondral lesions of the talar dome. Foot Ankle 1993 Jan;14(1):48-55.
84 McKay GD, Goldie PA, Payne WR, Oakes BW. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med 2001 Apr;35(2):103-8.
85 Thacker SB, Stroup DF, Branche CM, Gilchrist J, Goodman RA, Weitman EA. The prevention of ankle sprains in sports. A systematic review of the literature. Am J Sports Med 1999 Nov;27(6):753-60.
86 Verhagen EALM, van Mechelen W, de Vente W. The effect of preventive measures on the incidence of ankle sprains. Clin J Sports Med 2000;10(4):291-6.
87 Chandani VP, Harper MT, Ficke JR, et al. Chronic ankle instability: evaluation with MR arthrography, MR imaging and stress radiography. Radiology 1994;192:189-94.
88 Fujii T, Luo ZP, Kitaoka HB, An KN. The manual stress test may not be sufficient to differentiate ankle ligament injuries. Clin Biomech (Bristol , Avon ) 2000 Oct;15(8):619-23.
89 Glasgow MA, Jackson AM, Jamicson. Instability of the ankle after injury to the lateral ligament. J Bone Joint Surg 1980;62-B:196-200.
90 Hubbard TJ, Kaminski TW, van der Griend RA, Kovaleski JE. Quantitative assessment of mechanical laxity in the functionally unstable ankle. Med Sci Sports Exerc 2004;36(5):760-6.
91 Freeman MA. Treatment of ruptures of the lateral ligament of the ankle. J Bone Joint Surg Br 1965 Nov;47(4):661-8.
92 Perlman M, Leveille D, DeLeonibus J, et al. Inversion lateral ankle trauma: review of the literature, and prospective study. J Foot Surg 1987;26(2):95-135.
93 Wiklerson GB, Nitz AJ. Dynamic ankle instability: mechanical and neuromuscular interrelationships. J Sport Rehab 1994;3:43-57.
94 Green T, Refshauge K, Crosbie J, Adams R. A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprains. Phys Ther 2001;81:984-94.
95 Lankhorst GJ, Timmer M. Invaliditeitsen arbeids(on)geschiktheidsschattingen. Ned Tijdschr Geneeskd 1990;3:215-7.
96 Brunnekreef JJ, van Uden CJ, van MS, Kooloos JG. Reliability of videotaped observational gait analysis in patients with orthopedic impairments. BMC Musculoskelet Disord 2005 Mar 17;6(1):17.
97 Kaikkonen A, Kannus P, Jarvinen M. A performance test protocol and scoring scale for the evaluation of ankle injuries. Am J Sports Med 1994 Jul;22(4):462-9.
98 Haywood KL, Hargreaves J, Lamb SE. Multi-item outcome measures for lateral ligament injury of the ankle: a structured review. J Eval Clin Pract 2004 May;10(2):339-52.
99 Karlsson J, Peterson L. Evaluation of ankle joint function. The use of a scoring scale. Foot 1991;11:15-9.
100 Rose A, Lee RJ, Williams RM, Thomson LC, Forsyth A. Functional instability in non-contact ankle ligament injuries. Br J Sports Med 2000 Oct;34(5):352-8.
101 Cross KM, Worrel TW, Leslie JE, van Veld Kahlid R. The relationship between self-reported and clinical measures and the number of days to return to sport following acute ankle sprains. JOSPT 2002;32(1):23.
102 Hoiness P, Glott T, Ingjer F. High-intensity training with a bi-directional bicycle pedal improves performance in mechanically unstable ankles - a prospective randomized study of 19 subjects. Scand J Med Sci Sports 2003 Aug;13(4):266-71.
103 Beurskens AJ, de Vet HC, Köke AJ. Responsiveness of functional status in low back pain: a comparison of different instruments. Pain 1996 Apr;65(1):71-6.
104 Beurskens AJ, de Vet HC, Koke AJ, Lindeman E, van der Heijden GJ, Regtop W, et al. A patient-specific approach for measuring functional status in low back pain. J Manipulative Physiol Ther 1999 Mar;22(3):144-8.
105 Miller MD, Daron G, Feris MD. Measurement of subjective phenomena in primary care research: the visual analogue scale. Fam Pract Res J 1993;13:15-24.
106 Wevers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 13, 227- 236. 1990. Ref Type: Abstract
107 Howell DW. Therapeutic exercise and mobilisation. In: Hunt GC, editor. Physical Therapy of the foot and ankle. New York: Churchill Livingstone; 1988.
108 Prentice WE, Bell GW. Pathophysiology of musculoskeletal injuries and the healing process. In: Prentice WE, editor. Rehabilitation techniques in sports medicine. St. Louis: Times Mirror/Mosby College Publ; 1990.
109 Reed B, Zarro V. Inflammation and repair and the use of thermal agents. In: Michlovitz SL, editor. Thermal agents in rehabilitation. Philadelphia: FA Davis CO; 1986.
110 Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med 2004 Jan;32(1):251-61.
111 Cote DJ, Prentice WE, Hooker DN, et al. Comparison of three treatment procedures for minimizing ankle sprain swelling. Phys Ther 1988;68:1064-76.
112 Laba E. Clinical evaluation of ice therapy for acute ankle sprain injuries. NZ J Physiother 1989;17:7-9.
113 Michlovitz S, Smith W, Watkins M. Ice and high voltage pulsed stimulation in treatment of acute lateral ankle sprains. JOSPT 1988;9:301-4.
114 Sloan JP, Hain R, Pownall R. Clinical benefits of early cold therapy in accident and emergency following ankle sprain. Arch Emerg Med 1989;6:1-6.
115 Wilkerson GB, Horn-Kingery HM. Treatment of the inversion ankle sprain: comparison of different modes of compression and cryotherapy. JOSPT 1993;17:240-6.
116 Griffin JE, Karselis TC. Physical agents for physical therapists. Springfield, IL: Charles C Thomas Publ; 1978.
117 McMaster WC. Cryotherapy. Physician Sports Med 1982;10(11):112-9.
118 Cooper DL, Fair J. Contrast baths and pressure treatment for ankle sprains. Physician Sports Med 1979;7(4):143.
119 McCluskey GM, Blackburn TA, Jr., Lewis T. A treatment for ankle sprains. Am J Sports Med 1976 Jul;4(4):158-61.
120 Airaksinen O, Kolari PJ, Miettienen H. Elastic bandages and intermittent pneumatic compression for treatment of acute ankle sprains. Arch Phys Med Rehabil 1990;71(6):380-3.
121 Rucinsky JJ, Hooker DN, Prentice WE, Shields EW, et al. The effects of intermittent compression on oedema in postacute ankle sprains. JOSPT 1991;14(2):65-9.
122 Tsang KK, Hertel J, Denegar CR. Volume Decreases After Elevation and Intermittent Compression of Postacute Ankle Sprains Are Negated by Gravity-Dependent Positioning. J Athl Train 2003 Dec;38(4):320-4.
123 Kerkhoffs GMMJ, Handoll HHG, de Bie R, Rowe BH, Struijs PAA. Surgical versus conservative treatment for acute injuries of the lateral ligament complex of the ankle in adults. The Cochrane Library 2002.
124 Kerkhoffs GMMJ, Struijs PAA, Marti RK, Assendelft WJJ, Blankevoort L, van Dijk CN. Different functional treatment strategies for acute lateral ankle ligament injuries in adults. The Cochrane Library 2002.
125 Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly K, Struijs PA, van Dijk CN. Immobilisation and functional treatment for acute lateral ankle ligament injuries in adults. Cochrane Database Syst Rev 2002;(3): CD003762.
126 Munk B, Holm-Christensen K, Lind T. Long-term outcome after ruptured lateral ankle ligaments. A prospective study of three different treatments in 79 patients with 11-year follow-up. Acta Orthop Scand 1995 Oct;66(5):452-4.
127 Ogilvie-Harris DJ, Gilbart M. Treatment modalities for soft tissue injuries of the ankle: a critical review. Clin J Sport Med 1995;5:187-95.
128 Shrier I. Treatment of lateral collateral ligament sprains of the ankle: a critical appraisal of the literature. Clin J Sport Med 1995 Jul;5(3):187-95.
129 Verhagen EA, van der Beek AJ, van Tulder MW. The effect of tape, braces and shoes on ankle range of motion. Sports Med 2001;31(9):667-77.
130 Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial. Br Med J (Clin Res Ed) 1981 Feb;21;282(6264):606-7.
131 Klein J, Hoher J, Tilling Th. Comparative study of therapies for fibular ligament rupture of the lateral ankle joint in competitive basketball players. Foot & Ankle 1993;14:320-4.
132 Tropp H, Odenrick P, Gillquist J. Stabilometry recordings in functional and mechanical instability of the ankle joint. Int J Sports Med 1985 Jun;6(3):180-2.
133 Holme E, Magnusson SP, Becher K, Bieler T, Aagaard P, Kjaer M. The effect of supervised rehabilitation on strength, postural sway, position sense and re-injury risk after acute ankle ligament sprain. Scand J Med Sci Sports 1999 Apr;9(2):104-9.
134 van Os AG, Bierma-Zeinstra SM, Verhagen AP, de Bie RA, Luijsterburg PA, Koes BW. Comparison of conventional treatment and supervised rehabilitation for treatment of acute lateral ankle sprains: a systematic review of the literature. J Orthop Sports Phys Ther 2005 Feb;35(2):95-105.
135 van Os AG, Bierma-Zeinstra SM, Kleinrensink GJ, Bernsen RMD, Verhaar JAN, Koes BW. Effects of supervised exercises for adults with an acute lateral ankle sprain: a randomised clinical trial. submitted 2005.
136 Verhagen EALM, van der Beek AJ, Twisk JWR, Bouter LM, Bahr R, van Mechelen W. The effect of a proprioceptive balance board training programme for the prevention of ankle sprains. Am J Sports Med 2004;32(6):1385-93.
137 Bahr R, Lian O, Bahr IA. A twofold reduction in the incidence of acute ankle sprains in volleyball after the introduction of an injury prevention program: a prospective cohort study. Scand J Med Sci Sports 1997;7:172-7.
138 Eils E, Rosenbaum D. A multi-station proprioceptive exercise program in patients with ankle instability. Med Sci Sports Exerc 2001 Dec;33(12):1991-8.
139 Heidt RS, Jr., Sweeterman LM, Carlonas RL, Traub JA, Tekulve FX. Avoidance of soccer injuries with preseason conditioning. Am J Sports Med 2000 Sep;28(5):659-62.
140 Safran MR, Zachazewski JE, Benedetti RS, Bartolozzi AR, III, Mandelbaum R. Lateral ankle sprains: a comprehensive review part 2: treatment and rehabilitation with an emphasis on the athlete. Med Sci Sports Exerc 1999 Jul;31(7 Suppl):S438-S447.
141 Soderman K, Werner S, Pietila T, Engstrom B, Alfredson H. Balance board training: prevention of traumatic injuries of the lower extremities in female soccer players? A prospective randomized intervention study. Knee Surg Sports Traumatol Arthrosc 2000;8(6):356-63.
142 Barret DS. Proprioception and function after anterior cruciate reconstruction. J Bone Joint Surg 1991;73-B(5):833-7.
143 Brink PR, Runne WC, Wever J. Functional treatment of rupture of the lateral ligament of the ankle. Ned Tijdschr Geneeskd 1988 Apr 9;132(15):672-6.
144 Ferell WR, Baxendale RH, Carnachan C, et al. The influence of joint afferent discharge on locomotion, proprioception and activity in conscious cats. Brain Research 1985;347:41-8.
145 Freeman MA. Coordination exercises in the treatment of functional instability of the foot. Physiotherapy 1965;393-5.
146 Kottke FJ, Halpern D, Easton JKM, et al. The training of coordination. Arch Phys Med Rehab 1978;59:557-67.
147 Oostendorp RAB, van de Sande JAW. Arthrokinetische reacties en musculaire instabiliteit. Ned Tijdschr Fysiother 1983;93(2):63-72.
148 Trevino SG, Davis P, Hecht PJ. Management of acute and chronic lateral ligament injuries of the ankle. Orthop Clin North Am 1994 Jan;25(1):1-16.
149 Tropp H, Ekstrand J, Gillquist J. Stabilometry in functional instability of the ankle and its value in predicting injury. Med Sci Sports Exerc 1984;16(1):64-6.
150 Tropp H, Ekstrand J, Gillquist J. Factors affecting stabilometry recordings of single limb stance. Am J Sports Med 1984 May;12(3):185-8.
151 Blackburn T, Guskiewicz KM, Petschauer MA, Prentice WE. Balance and joint stability: The relative contributions of proprioception and muscular strength. J Sport Rehab 2000;9:315-28.
152 Hoffman M, Payne VG. The effects of proprioceptive ankle disk training on healthy subjects. J Orthop Sports Phys Ther 1995 Feb;21(2):90-3.
153 Waddington G, Adams R, Jones A. Wobble board (ankle disc) training effects on the discrimination of inversion movements. Aust J Physiother 1999;45(2):95-101.
154 Bernier JN, Perrin DH. Effect of coordination training on proprioception of the functionally unstable ankle. J Orthop Sports Phys Ther 1998 Apr;27(4):264-75.
155 Matsusaka N, Yokoyama S, Tsurusaki T, Inokuchi S, Okita M. Effect of ankle disk training combined with tactile stimulation to the leg and foot on functional instability of the ankle. Am J Sports Med 2001;29(1):25-30.
156 Stomp DJ, Hendriks HJM, Heemskerk MAMB, van der Wees PhJ, de Bie RA. Effectiviteit van fysiotherapie bij patiënten met chronische functionele instabiliteit van de enkel: een systematisch literatuuroverzicht. Ned Tijdschr Fysiother 2005;115(2):26-31.
157 van der Wees PhJ, Lenssen AF, Hendriks HJM, Stomp DJ, Dekker J, de Bie RA. Effectiveness of exercise therapy and manual mobilisation in acute ankle sprain and functional instability: a systematic review. Aust J Physiother 2006;52:27-37.
158 Stasinopoulos D. Comparison of three preventive methods in order to reduce the incidence of ankle inversion sprains among female volleyball players. Br J Sports Med 2004;38:182-5.
159 Sheth P, Yu B, Laskowski ER, An KN. Ankle disk training influences reaction times of selected muscles in a simulated ankle sprain. Am J Sports Med 1997 Jul;25(4):538-43.
160 Wojtys EM, Wylie BB, Huston LJ. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am J Sports Med 1996 Sep;24(5):615-21.
161 Hess DM, Joyce CJ, Arnold BL, Gansneder BM. The effect of a 4-week agility-training program on postural sway in the functionally unstable ankle. J Sport Rehabil 2001;24(1):17-24.
162 Powers ME, Buckley BD, Kaminski TW, Hubbard TJ, Ortiz C. Six weeks of strength and proprioception training does nof affect muscle fatigue and static balance in functional ankle instability. J Sport Rehabil 2004;13(3):201-27.
163 Gandevia SC, McCloskey DI, Burke D. Kinaesthetic signals and muscle contraction. Trends Neurosci 1992 Feb;15(2):62-5.
164 Uh BS, Beynnon BD, Helie BV, Alosa DM, Renstrom PA. The benefit of a single-leg strength training program for the muscles around the untrained ankle. Am J Sports Med 2000 Jul;28(4):568-73.
165 Docherty CL, Moore JH, Arnold BL. Effects of strength training on strength development and joint position sense in functionally unstable ankles. Journal of Athletic Training 1998;33(4):310-4.
166 Collins N, Teys P, Vincenzino B. The initial effects of Mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains. Manual Therapy 2004;9:77-82.
167 Pellow JE, Brantingham JW. The efficacy of adjusting the ankle in the treatment of Subacute and Chronic Grade I and Grade II Ankle Inversion Sprains. Journal of Manipulative and Physiological Therapeutics 2001;24(1).
168 Eisenhart AW, Gaeta TJ, Yens DP. Osteopathic Manipulative Treatment in the emergency department for patients with acute ankle injuries. J Am Ostheopath Assoc 2003;103(9):417-21.
169 Gezondheidsraad. De effectiviteit van fysische therapie: elektrotherapie, lasertherapie, ultrageluidbehandeling. Den Haag: Gezondheidsraad; 1999.
170 van der Windt DAWM, van der Heijden GJMG, van den Berg SGM, ter Riet R, de Winter AF, Bouter LM. Ultrasound Therapy for acute ankle sprains. 2002.
171 de Bie RA, de Vet HC, Lenssen T, van den Wildenberg FA, Kootstra G, Knipschild PG. Low-level laser therapy in ankle sprains: a randomized clinical trial. Arch Phys Med Rehabil 1998;79(11):1415-20.
172 de Bie RA. Efficacy of 904 nm laser therapy in acute lateral ankle sprains. Maastricht: Maastricht University; 1998.
173 Barker AT, Barlow PS, Porter J, Smith ME, et al. A double-blind clinical trial of lower power pulsed shortwave therapy in the treatment of a soft tissue injury. Phys Ther 1985;71(12):500-4.
174 Pasila M, Visuri T, Sundholm A. Pulsating shortwave diathermy: value in treatment of recent ankle and foot sprains. Arch Phys Med Rehabil 1978 Aug;59(8):383-6.
175 Pennington GM, Danley DL, Sumko MH, Bucknell A, Nelson JH. Pulsed, non-thermal, high-frequency electromagnetic energy (DIAPULSE) in the treatment of grade I and grade II ankle sprains. Mil Med 1993 Feb;158(2):101-4.
176 Wilson DH. Treatment of soft-tissue injuries by pulsed electrical energy. Br Med J 1972;2:269-70.
177 Handoll HHG, Rowe BH, Quinn KM, de Bie R. Interventions for preventing ankle ligament injuries. The Cochrane Library 2001.
178 Sitler M, Ryan J, Wheeler B, McBride J, Arciero R, Anderson J, et al. The efficacy of a semirigid ankle stabilizer to reduce acute ankle injuries in basketball. A randomized clinical study at West Point. Am J Sports Med 1994 Jul;22(4):454-61.
179 Vaes PH, Duquet W, Van Gheluwe B. Werkzaamheid van enkelbandages en enkelortheses. Jaarboek Fysiotherapie. 2000. p. 49-66.
180 Garrick JC, Requa RK. Role of external support in the prevention of ankle sprains. Med Sci Sports 1973;(5):200-3.
181 Gross MT, Lapp AK, Davis M. Comparison of Swede-O-Universal ankle support and Aircast Sport-Stirrup orthoses and ankle tape in restricting eversion-inversion before and after exercise. JOSPT 1991;13:11-9.
182 Gross MT, Ballard CL, Mears HG, Watkins EJ. Comparison of Donjoy ankle ligaments protector and Aircast Sport-Stirrup orthoses in restricting foot and ankle motion before and after exercise. JOSPT 1992;16:60-7.
183 Gross MT, Everts JR, Roberson SE, Roskin DS, Young KD. Effect of Donjoy Ankle Ligament Protector and Aircast Sport-Stirrup orthoses on functional performance. JOSPT 1994 Mar;19(3):150-6.
184 Hamer PW, Munt AM, Harris CD, James NC. The influence of ankle strapping on wobbleboard performance, before and after exercise. Aust J Physiother 1992;38:85-92.
185 Firer P. Effectiveness of taping for the prevention of ankle ligaments sprains. Br J Sports Med 1990;24:47-50.
186 Karlsson J, Sward L, Andreasson GO. The effect of taping on ankle stability. Practical implications. Sports Med 1993 Sep;16(3):210-5.
187 Lohrer H, Alt W, Gollhofer A. Neuromuscular properties and functional aspects of taped ankles. Am J Sports Med 1999 Jan;27(1):69-75.
188 Manfroy PP, Ashton-Miller JA, Wojtys EM. The effect of exercise, prewrap, and athletic tape on the maximal active and passive ankle resistance of ankle inversion. Am J Sports Med 1997 Mar;25(2):156- 63.
189 Refshauge KM, Kilbreath SL, Raymond J. The effect of recurrent ankle inversion sprain and taping on proprioception at the ankle. Med Sci Sports Exerc 2000 Jan;32(1):10-5.
190 Glick JM, Gorden RB, Nishimoto D. The prevention and treatment of ankle injuries. Am J Sports Med 1976;4:136-41.
191 Rarick GL, Bigley G, Karst R, Malina RM. The measurable support of the ankle joint by conventional methods of taping. Am J Orthop 1962 Sep;44-A:1183-90.
192 van Wingerden BA. Tape en bandagetechnieken. Lochem: De Tijdstroom; 1982.
193 Riezebos C, Lagerberg A. Inversietrauma van de enkel, ontstaansmechanismen, risicofactoren en preventie. Ned Tijdschr Fysiother 1998;16:16-47.
194 Alves JW, Alday RV, Ketcham DL, Lentell G. A comparison of the passive support provided by various ankle braces. JOSPT 1992;15:10-8.
195 Beynonn BD, Renstrom PA. The effect of taping and bracing in sports. Ann Chir Gyneacol 1991;80:230-8.
196 Johnson RE, Veale JR, McCarthy GJ. Comparative study of ankle support devices. J Am Podiatr Med Assoc 1994 Mar;84(3):107-14.
197 Shapiro MS, Kabo JM, Mitchell PW, Loren G, Tsenter M. Ankle sprain prophylaxis: an analysis of the stabilizing effects of braces and tape. Am J Sports Med 1994 Jan;22(1):78-82.
198 Stiggelbout M, van Mechelen W. De preventiewaarde van de enkelbrace in vergelijking tot enkeltaping ter voorkoming van enkeldistorsies bij sporters. Geneesk Sport 1993;26(1):10-7.
199 Brunch RP, Bednarski K, Holland D. Ankle joint support: a comparison of reusable lace-on braces with taping and wrapping. Phys Sport Med 1985;13:59-62.
200 Hughes LH, Stetts DM. A comparison of ankle taping and semirigid support. Phys Sport Med 1983;11:99-103.
201 Leemrijse C. Gaat bij chronische instabiliteit van de enkel de voorkeur uit naar bandageren/tapen of pushbraces? Respons 1990;1:1-2.
202 Rovere GD, Clarke TL, Yates CS, et al. Retrospective comparison of taping and ankle stabilizers in preventing ankle injuries. Am J Sports Med 1988;16:228-33.
203 Barret JR, Tanji JL, Drake C, et al. High- versus low-top shoes for the prevention of ankle sprains in basketball players. A prospective randomized study. Am J Sports Med 1993;21(4):582-5.
204 van Mechelen W, Hlobil H, Kemper HC, Voorn WJ, de Jongh HR. Prevention of running injuries by warm-up, cool-down, and stretching exercises. Am J Sports Med 1993 Sep;21(5):711-9.
205 Pope RP, Herbert RD, Kirwan JD, Graham BJ. A randomized trial of pre-exercise stretching for prevention of lower-limb injury. Med Sci Sports Exerc 2000 Feb;32(2):271-7.
Algemene informatie
- Alle aanbevelingen
- Inleiding
- A.1 Doelstelling en doelgroep
- A.2 Acuut enkelletsel versus functionele instabiliteit
- A.3 Klinische vraagstellingen
- A.4 Epidemiologische gegevens
- A.5 Prognostische factoren
- A.6 Etiologie van functionele instabiliteit
- A.7 Screeningsproces
- A.7.1 Differentiaaldiagnostiek
- A.7.2 Informeren en adviseren
Diagnostisch proces
- Inleiding
- B.1 (Aanvullende) anamnese
- B.2 (Aanvullend) onderzoek
- B.3 Meetinstrumenten
- B.4 Analyse
- B.5 Conclusie
Therapeutisch proces
- Inleiding
- C.1 Acuut enkelletsel
- C.1.1 Doelstellingen
- C.1.2 Verrichtingen bij acuut enkelletsel
- C.1.2.1 IJs en compressie in de ontstekingsfase na acuut enkelletsel
- C.1.2.2 Functioneel behandelen na acuut enkelletsel
- C.1.2.3 Oefentherapie
- C.1.2.4 Spierkrachttraining
- C.1.2.5 Manuele mobilisatie
- C.1.2.6 Fysische therapie in engere zin
- C.2 Functionele instabiliteit van de enkel
- C.2.1 Doelstellingen bij functionele instabiliteit
- C.2.2 Verrichtingen bij functionele instabiliteit
- C.2.3 Evaluatie
- C.3 Preventie van enkelletsel
- C.3.1 Preventieve werking van tape en brace
- C.3.2 Preventieve werking van schoeisel
- C.3.3 Preventieve werking van warming-up en cooling-down
- C.4 Tijds- en doseringsindicaties
- C.5 Afsluiting en verslaglegging